
Alcohol: Good or Bad? Why Reductionist Science Can't Answer a Complex Social, Nutritional Question
If you are reading about NADPH and neutral circuits you aren't even close to thinking about it correctly

Recently, I tweeted something to the effect that changing your alcohol consumption based on short term studies that measure dubious surrogate endpoints is a fool’s errand, and I stand by that. Indeed, for something as complex as drinking, making personal choices by measuring a handful of metabolites (neural circuits or seratonin or nadph+) is an impoverished way of thinking about your life.
When it comes to a complex social and nutritional intervention like alcohol consumption, the best scientific evidence is woefully inadequate. First, there are at least 4 endpoints that matter when it comes to guiding your alcohol intake.
How long will I live?
How well will I live (morbidity/ disability)?
How happy will I be/ How will I feel?
How happy are people around me/ How will they feel?
Next, we don’t enter as tabula rasa, but as complex human beings with habits and customs. We all start with a different baseline. Some of us prefer to drink 0, 1, 2, 3 or 4+ drinks per day. That’s the baseline. How we each are living right now.
Then, to make it more complex, consider that just as eating carrots and drinking coke are not the same action; drinking a shot of cheap vodka, a fine Gamay from Switzerland, a glass of St Bernardus Abt12, are not the same form of consumption. Yet nearly all studies reduce this into “grams of alcohol per day.”

Furthermore, there may be additional interactions we don’t yet know are salient. Such as drinking in a hot climate might be different than a cold one, drinking with others might be different than drinking alone, drinking with certain foods might be different than drinking with none.
When you think about all this complexity, and want to leverage science to better understand the issue, the best study to move the ball forward I can envision is the following.
We enroll people with their current preferred baseline drinking (0,1,2,3,4, etc.). We randomize them into one of 7 arms.
Arm 1: Stay the course
Arm 2: Decrease your drinking by 1 drink a day (advice given)
Arm 3: Increase your drinking by 1 drink a day
Arm 4: Decrease your drinking by 2
Arm 5: Increase your drinking by 2
Arm 6: Stop all drinking
Arm 7: Carpe diem (only advice provided)
Then, we follow people into the future. First, we measure the impact of our intervention on drinks consumed. Of course, like all complex social behavioral interventions, we won’t have perfect compliance, and that is ok. Our policy tests whether one recommendation is preferable to another. First step is to see what delta (drink consumption) we get from recommendations.
Next, we follow people into the future and look at all the relevant endpoints. If we enroll many people 65+, we may, in a few years, have some mortality data. I suspect it will generally be null. We may also have disability data (related to strokes, suicides, etc.). Again it is likely to be null. But the two most important endpoints: How you feel about your life, and how others feel about you will be continually captured. We will provide surveys to individuals, or have a diary tracking mood.
Because it is difficult for modest changes in nutrition to change duration of life and disability, the last 2 endpoints will likely drive the entire study (I.e will provide the most information to help you).
Put another way: I bet the most informative thing about the study will be how people feel about drinking more or less, and how others feel about them.
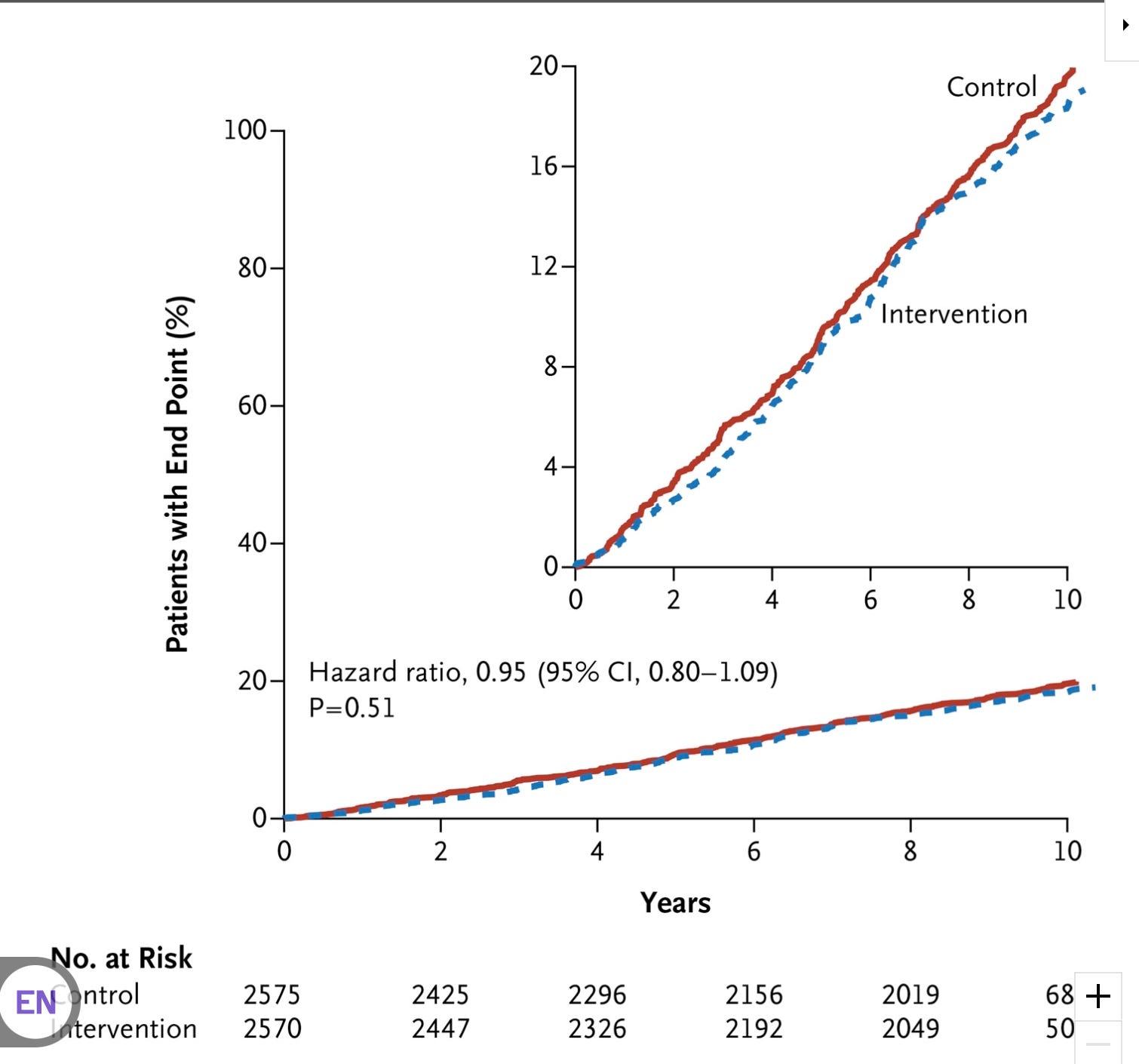
Why do I feel this way. Consider the massive NIH study Look Ahead. It randomized high risk, obese type 2 diabetes to intensive diet and exercise. And across all surrogates it succeeded spectacularly.

Of course, the primary endpoint was composite cardiovascular events, and that was… totally null. Just superimposable curves
I suspect my 7 arm trial will be like this for mortality, and composite measures of disability. I think the human satisfaction outcomes will drive the outcome.
In short, there is an appetite for advice about alcohol consumption. This leads many “scientists” to put forth recommendations about how much to drink, when and how. To bolster their case, they rely on flawed studies with short term endpoints. Mechanistic science is entirely in this camp. It is irrelevant what happens to synapses, cortical matter, mRIs, seratonin and other neurotransmitters.
Moreover, there is incentive to give advise people find palatable. In our puritanical nation, there is a strong minority who crave teetotaling advice. Perhaps this is the opposite in a culture like Russia. Yet, nearly all of this advice fails to capture the relevant things people care about when making a decision to drink or not to drink. Most advice fails to consider that most adults have already established their own equilibrium, and thus advice must begin with that starting point.
The study I propose is not perfect. One can imagine many more arms that specify the type of alcohol, maybe even provide it. Good IPAs, nice full bodied reds, or Belgian quadruple ales might be possible interventions. Who says the effect of alcohol is the same? Probably thats as silly as think 100 calories of Cheetos is the same as an apple.
Yet, despite my trials limits it is a vital first step in elevating alcohol literature from the evidence based gutter where it currently sits. Moreover, the NIH almost ran something like this, sadly that process was corrupted by the alcohol industry. These studies should be run by non conflicted parties.
Finally, among the limits: People who choose to sign up for my study are those willing to take suggestions about their alcohol use, which is a unique subset; however, these are the same people who listen to topical science podcasts and crave advice. The target population of people to advice are those who want advice.
In short, we know nearly nothing about how to advise alcohol use. I tweeted, “Advising people who don't drink to start drinking daily is silly and unproven, and advising people who are drinking a little bit each day to stop is silly and unproven.”
I think doctors and scientists should stay out of the debate; Push for the right studies, but I worry that instead we just get too many people with an opinion thats no better than no data at all.
VP. Points well taken, yet I sometimes feel that not every question is answered by what can only be an imperfect study. You ask doctors and scientists to stay out of the debate, yet you place yourself smack in the middle of it. As a doctor I’m entitled to my opinion based on the data I see plus my individual observations. Your approach should also include tobacco. The health hazards of smoking did not reveal themselves from a randomized study, yet one can also conclude that many people enjoy smoking and do not get sick or live less. Finally, the missing piece in your proposed study is individual genetic variance in how we metabolize alcohol, likely a defining factor for how our diets affect us.
If I have a few glasses of a Glenfiddich with friends, I get funnier, some say wittier. For sure I get better looking. My points on literature and art and music and films become more insightful, my personal stories much deeper and lucid. My friends, and any women in the room want to know more about me. A few whiskies with ice in a proper crystal tumbler are the perfect social lubricant.
Now about that study on drinking. What are you trying to uncover? I'm sorry, your point is?