
Clarifying a few misconceptions about lung cancer screening

I received a few notes from readers, and some comments are worth further clarification and education.
If lung cancer screening DID NOT improve mortality but DID make surgeries smaller, led to less chest tubes, led to less ports, led to less chemotherapy— that would be worthwhile, and is a reason to screen.
This is true, but the problem is there is no evidence that lung cancer screening does any of these things. If you think there is evidence for this, please link to it below. The authors of NLST and Nelson have access to (or could obtain) the FULL data on downstream procedures and have never reported them. Some reports include only the FIRST downstream procedure. I would support screening if it could improve these endpoints but there is no evidence it does. There is in fact no paper on the topic in lung cancer. The lung cancer trials don’t tell us how many people got chemo or surgery or how big the surgeries were etc. Yet, Welch did look at this for breast cancer. At least for breast cancer the truth was counterintuitive. Here is SEER data.
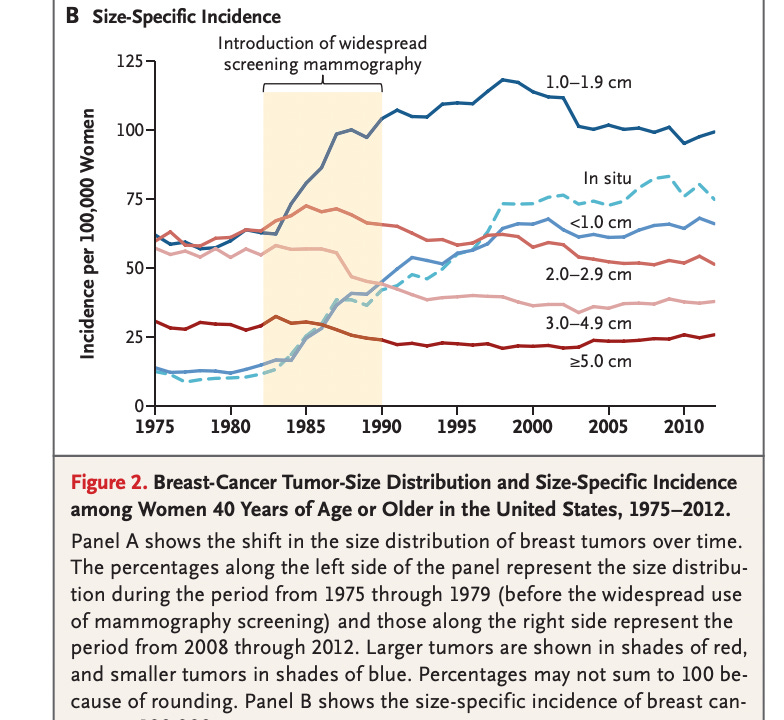
If breast cancer screening means finding small tumors that were going to get big, and sparing you a larger surgery or chemotherapy, you would expect the rise in small tumors being diagnosed to be offset by a commensurate and delayed reduction in large tumors. Yet this is not the case, there is no reduction in large tumors at all. This suggests mammograms find way more small tumors and does nothing to stop denovo metastatic disease (other Welch paper) or large tumors. With CT screening for lung cancer, there is no evidence to date. I am open to being persuaded, and the best way to do that is to email the RCT authors and ask them to publish this. Why wouldn't they, if it's so wonderful?
Lung cancer specific mortality is a better endpoint than all cause mortality, some argue. I disagree, and a simple story will illustrate why. A 74 yo gets screened for lung cancer and they find a small mass. A CT guided needle biopsy results in pneumothrorax, and unfortunately the patient codes then and there. He can not be resuscitated. These events— or other complications, such as patient dies after EBUS or VATS are NOT COMMON— read that again, they are NOT COMMON— but they are not zero. Lung cancer specific mortality does not count these events at all. There is no attempt to quantify the harms of screening on all downstream deaths in any cancer RCT — besides… of course… reliance on all cause mortality, which automatically captures all events. The fact the trials are stone cold negative for all cause mortality should be disclosed to patients.
When I was in fellowship, there was a poor patient with Hodgkin’s lymphoma whom the attending blasted with chemotherapy— extremely high doses. The drugs eventually caused liver failure, and the patient died. The attending said, “at least he didn’t die of lymphoma.” I am not persuaded by such arguments.