
COVID19 influencers again promote flawed paper
A JACC paper does not prove vax lowers MACE after a covid infection| Influencers misinterpret it

Dr Eric Topol once again is promoting bad science. Sadly, this time, his promotion has earned over 1000 retweets. Let’s take a close look at the study and why it is wrong. But first, here is the tweet.

This paper in question comes from the Mt. Sinai investigators, a point I will return to. Basically it claims that vaccination lowers the risk of major adverse cardiovascular events— which typically includes acute myocardial infarction (AMI), stroke, and cardiovascular mortality— after infection with sars-cov-2 documented in the EHR. You were considered vaccinated 2 weeks after your last dose, and you had to have sars-cov-2 documented in the EHR to be in this study.
Topol’s tweet misses the part that this is after EHR documented infection, not “during follow up”. MACE events that occurred without prior covid 19 are not included.
Why am I not surprised he missed this?
What does it mean to have COVID in the EHR? That comes from a linked paper. But basically you had to have a COVID19 code the dataset, but could have even tested negative for COVID. What a joke!
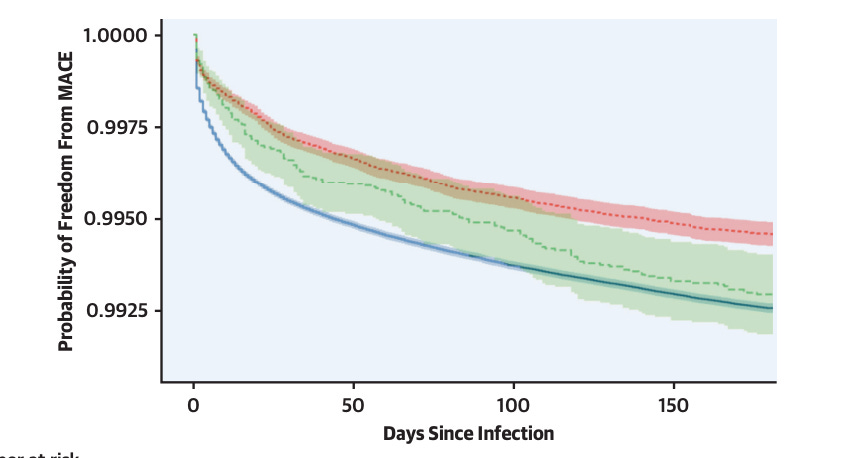
Once this code is placed in the chart, the authors see when MACE codes occur. Check it out. The answer is immediately. It occurs immediately more often in the unvax’d.
Because you were unvaccinated, you immediately have a heart attack when you get COVID— is the authors claim.
Is this true? Is this likely? Are there competing explanations?
In order to be in this dataset you have to have documented COVID19 in an EHR. The reasons vaccinated and unvaccinated people seek medical care is not known and may vary. The vaccinated person might be presenting with COVID19 with a mild cough and looking for paxlovid or other medical advice; the unvax’d person might be presenting to the hospital with a heart attack and then only incidentally found to have COVID19. Almost surely this is what is happening disproportionately. We know unvaccinated people are different in ways apart from vaccination, which I will return to.
The authors limits include blah-blah the usual boilerplate, but they do not mention the biggest limit. The paper assumes that unvaccinated and vaccinated people are seeking medical care for covid and apart from covid ENTIRELY EQUALLY— which is almost surely not true.
The time course of the result is more plausibly explained by different health care seeking behavior. And we know unvaccinated people behave differently. They even have more car accidents! PS I demolish that paper here. It is simple to assume these results are driven by incidental COVID19 for the presentation of a heart attack, which occurs more often. And no evidence is presented to challenge this hypothesis.
Does vaccination lower heart attacks post COVID breakthrough itself? That is a harder question that this paper cannot answer.
One more point. Even among the unvaccinated. Even if they have a documented COVID19 infection in an EHR 99.25% don’t have MACE in 180 days. Can we chillax, pls?
Other researchers clearly get it:

PS: I remember some on this team of observational researchers.
A team from Mt. Sinai with overlapping authors published an uncontrolled study of anti-coagulation during the heat of the pandemic, while simultaneously declining to participate in a randomized trial. I documented that here. They changed a protocol in the hospital for 5000 people without running a controlled study. This was sad times. It was wrong to experiment on people without learning anything. Please read this thread.
A quick look at Topol's bio provides an interesting hypothesis regarding his willingness to ditch science in order to support the pro-vax-mandate narrative:
(from wikipedia): He is the founder and director of the Scripps Research Translational Institute, a professor of Molecular Medicine at The Scripps Research Institute, and a senior consultant at the Division of Cardiovascular Diseases at Scripps Clinic in La Jolla, California.
Scripps is Fauci/NIH's number one research partner.
How much money did Topol and Scripps get from the NIH in recent years?
(more wikipedia): In 2016, Topol was awarded a US$207 million grant from the National Institutes of Health to lead a significant part of the Precision Medicine Initiative
This is in addition to his role as principal investigator for a $35M grant from the National Institutes of Health to promote innovation in medicine and the education and career training of future medical researchers.
So Topol/Scripps received at least a quarter of a billion dollars from NIH since 2016!
What are Topol's specialty areas?
(from his Scripps bio page) His principal scientific focus has been on the use of genomic and digital data, along with artificial intelligence, to individualize medicine. He is also a practicing cardiologist.
A very brief scroll through his publications on Google scholar suggests that he did cardiology-related research in the years prior to his job/s at Scripps (pre-2006), but has focused almost exclusively on the future of medicine (genomics, digital data, AI etc.) since then. Then, when Covid hit, he suddenly became interested in research supporting the NIH's Covid narrative. Not just about Covid and cardiac events, but also things like "Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review" -- WHAT???? HOW DOES THAT FIT INTO ANY OF HIS AREAS OF RESEARCH/EXPERTISE????
One of Topol's Scripps colleagues, Dr. Kristian Andersen, notoriously pointed out (in FOIAed emails) that SARS-CoV-2 looked like it could be engineered, and then did a 180 two days later and signed onto the natural origins paper. (https://www.nature.com/articles/s41591-020-0820-9).
Subsequently, Scripps received another $60M+ from the NIH
Does anyone have any doubt as to what's going on here?
Very sad that Topol closed his comment section permanently the day after he joined Substack.
Showed me he is pefers anti science.