
Do GLP-1 drugs reduce the risk of cancer?
A new observational study in the Annals of Oncology and a recent meta-analysis of randomized trials seem to offer different results

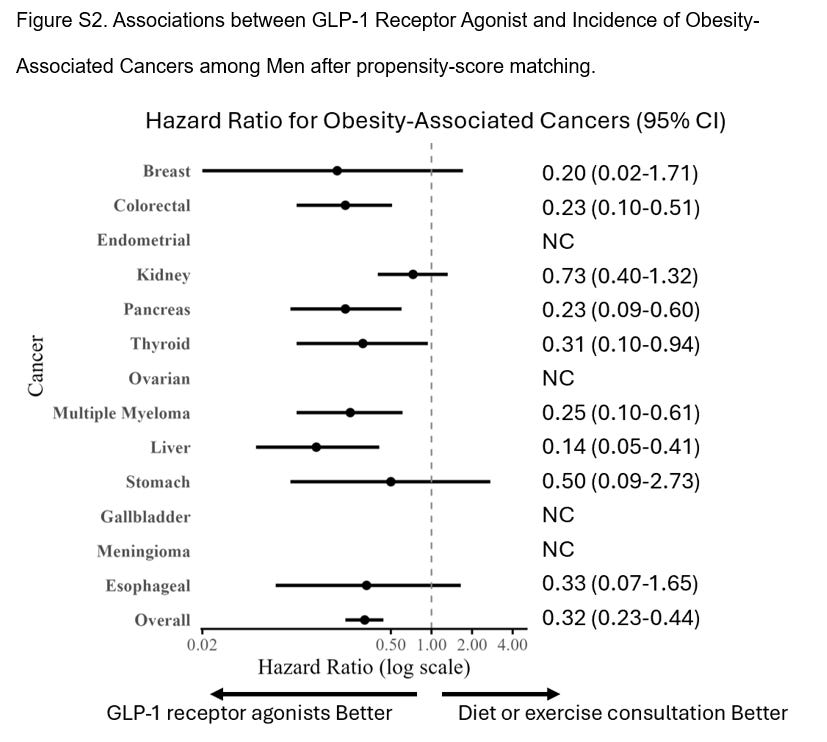
A new observational study— using “target trial” emulation— claims that in 2 years, GLP-1 lower the risk of cancer. It is being widely celebrated online. Bye bye myeloma, the authors would have you believe. Take a look.
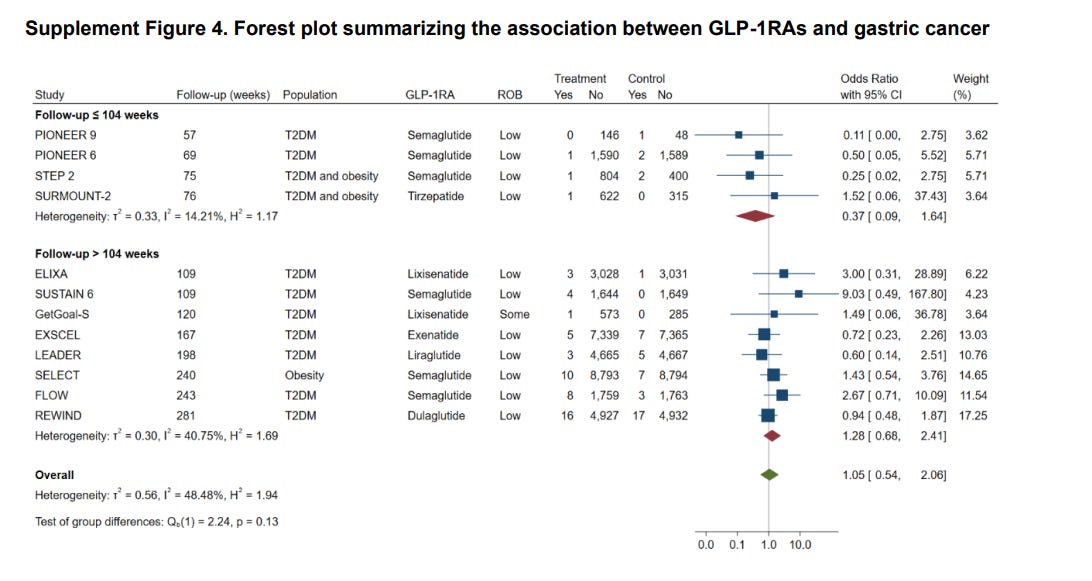
Yet, strangely, these results aren’t the case if you look at long term follow up of the randomized studies. Remember unlike a “target trial” a randomized trial is actually that— a trial. Prospectively designed, where the two groups have equalized outcome distributions in the absence of therapeutic effect, and time zero is set in stone. In other words, gold standard science. Take a look here.
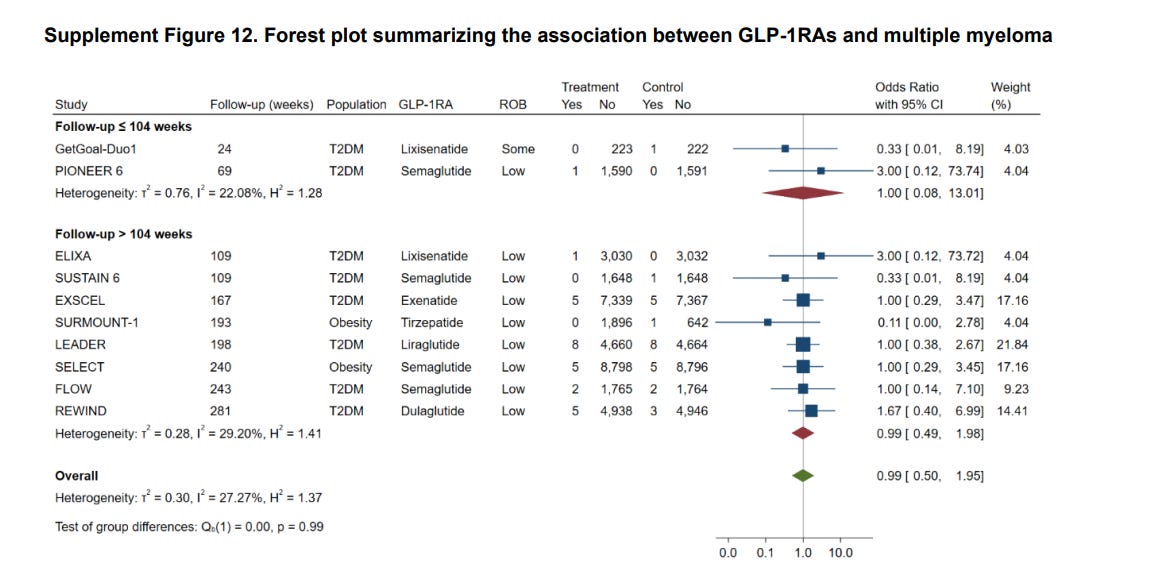
And as for myeloma….
What is this…. thyroid cancer is higher…
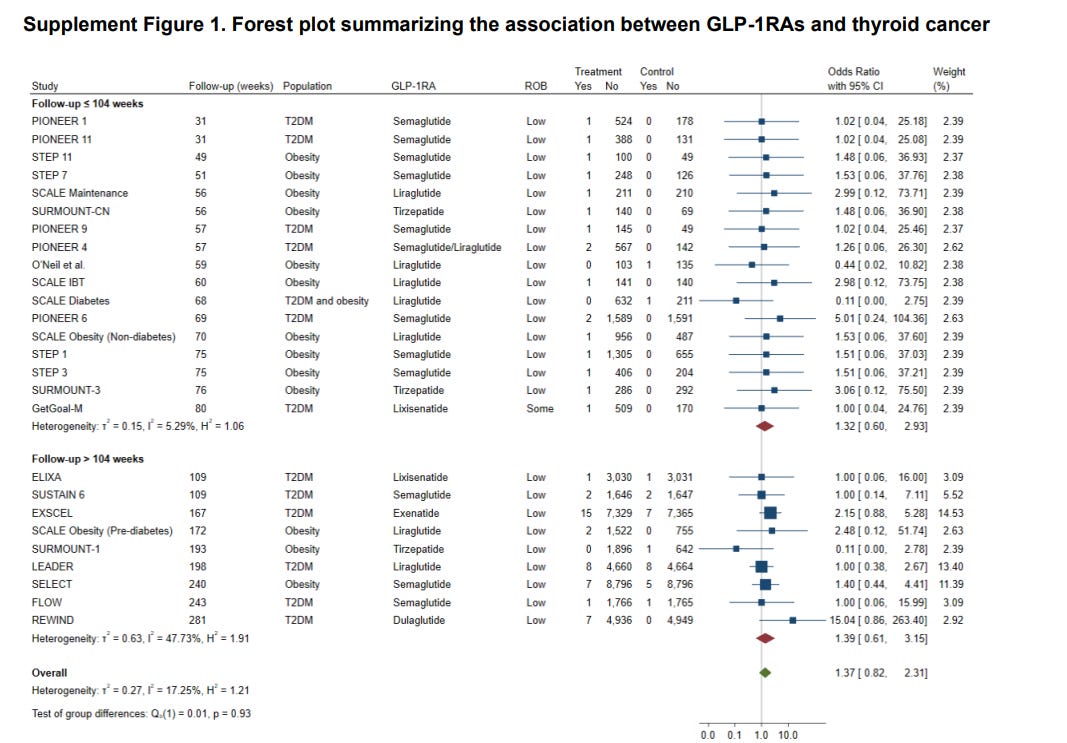
Thyroid cancer: it is notable that FDA requires a boxed warning here for a different reason… because these drugs can cause medullary thyroid cancer in animals.
The pooled effect in RCTs is confirmed by another meta-analysis I found.

Why are these results different?
Why does a recent observational study show these drugs prevent cancer, but the randomized trials don’t find that signal.
Option 1: There is not enough time in the randomized studies to see the benefit.
This can’t be the reason because the “target trial” has only a median of 2 year with IQR of 1 to 2 years of follow up. The target trial is as brief as some of the long term RCT follow up above.
Option 2: The observational “target trial” study has more power.
Maybe, but probably not a lot more power. The meta-analysis of RCTs has 90k participants, and the target trial is 80k vs 80k. I don’t have enough numerical info in the second paper to calculate power sadly. At first glance, it doesn’t look like there is a huge difference here.
Option 3: The target trial framework, like so much observational causal research, fails.
This has to be a leading possibility because even with the methods of target trial, emulations have failed to always predict randomized trials. The concordance rate is not much better than other methods. This was shown in an FDA funded project in JAMA.
Cancer takes far longer to develop than 2 years, so the overall finding in the new paper is preposterous on face value.
Option 4: The randomized data has other artifacts like control arm crossover or contamination, which biases to the null.
I searched and could not find the crossover rates. Maybe.
Overall: I think it is possible that these drugs will reduce cancer due to weight loss, but this recent annals of oncology paper is unlikely to be true.. At a minimum, the effect has not been seen in comparable randomized data.
It will take longer follow up and better data to make this case.
If you enjoy this Substack, subscribe
It makes sense to me that the drugs can reduce cancer if cancer risk increases with uncontrolled diabetes or insulin resistance. For the same reason people are losing weight - you've got the insulin resistance under control.
However, the question becomes whether there are other downsides (osteoporosis for example) or downsides of long-term exposure. The other question is whether people are using the time on GLP1s to successfully reprogram their habits. If not, the weight will just come right back, and so will your cancer risk.
Propensity-score analyses scare me. They aren't a replacement for randomization & always seem to overstate, but for whatever reason it seems they are read as "almost as good" as an RCT even though they can only compare on the stated variables, so you can never attribute the change to the intervention as in an RCT. Plus, how do you compare these patients? "Diet/exercise counseling," could be the doctor saying "you need to exercise" during a visit, & you have no idea if they did it or not. Versus GLP-1 users, who I imagine have much higher "patient activation" or engagement. You have to fight your insurance company to get an expensive drug & then inject it every week compared with Yeah right, I need to lose weight. So many other red flags.