
Long term cardiovascular complications of COVID
I examine the nature medicine paper

There are several questions that people want to know the answer to:
If I have been vaccinated and/or boosted and I get breakthrough COVID19 do I have to worry about long term cardiovascular (CV) complications?
If I got COVID19 prior to vaccination, do I have to worry about long term CV complications compared to if I hadn’t gotten COVID?
If I got COVID19 pre-vax do I have to worry about long term CV complications any more than someone who recovered from Influenza in years prior?
How much resources do we need to set aside for helping COVID19 survivors in years to come?
The funny thing is that this new Nature Medicine paper cannot answer any of these questions, though that does not stop errant interpretations online. The paper is entitled Long-term cardiovascular outcomes of COVID-19, and is getting widespread publicity. Let me briefly explain the paper, 3 key reasons for the results, and why it cannot address these 4 questions.
Here is what they did. Authors pulled Veterans Administration records to find 155k people who survived 30 days after a covid diagnosis. We have no idea how these diagnoses were made, but presumably they were all made 1. at the time of encountering the medical system (routine swab/ with covid), or 2. prompting encounter to medical system (felt sick/ from covid). The study does not include people who had COVID19 and never sought testing (—this would need seroprevalence to establish the cohort) or got tested elsewhere and recovered (missing from dataset). This is important because these latter 2 categories fit a lot of Americans who are curious about their risks (they had covid and either didn’t get tested, got home tested, or got tested outside their primary health care network). More to come on this.
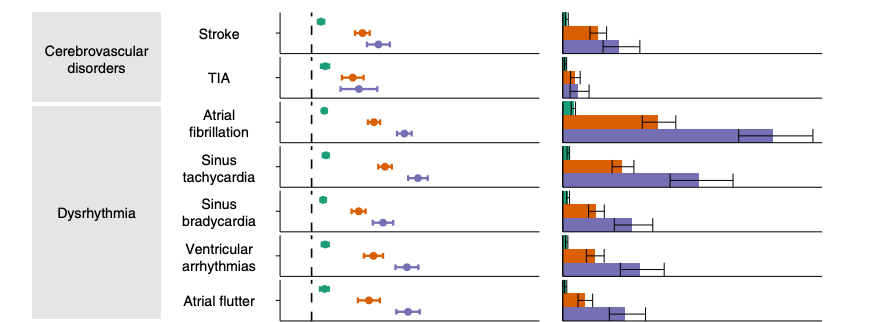
Compared to inverse probability weighted controls (at 2 time points), COVID19 survivors had more cardiovascular diagnoses in the months that followed. You have all seen the scary figure, here is a version of it. The relative risks are much larger than the absolute risks.
Of course, there are 3 reasons why people with a covid diagnosis have more subsequent cardiovascular (CV) issues in the electronic record than those without:
More cv issues were caused by covid
People who got covid get more tests/ more doctors pressing billing codes into their record
Despite IPW controls, people who had covid are vulnerable in ways not captured in the record. That is both why they got Covid, and why they went on to have bad CV things happen to them in greater numbers.
Despite the authors use of controls, they are not able to fully disambiguate these possibilities. Comparing pre-post covid diagnosis does not help, because the ensnarement effect (more testing) will only exist post-diagnosis. Negative disease (or falsification) controls are insufficient because they are unrelated to both cardiovascular disease and risk factors for getting COVID19 in the first place. We need negative controls related to CV risk but not related to getting covid. Good luck finding those!
Returning to our 4 questions
If I have been vaccinated and/or boosted and I get breakthrough COVID19 do I have to worry about long term cardiovascular (CV) complications?
This study used a data cut off of Jan 15 2021, likely nearly no one in the dataset had been vaccinated prior to getting covid (or very very few people). These data apply to what covid does to an unvaccinated person who presents to medical care at a Veterans Hospital prior to vaccine, and no other group. It does not apply to Omicron. It does not apply to breakthrough infections. After all the mantra is the breakthrough would have been worse if not for vax, by that logic, even if these increased risks are causal, it will all be less post vax. Moreover, the absolute risks are often so low no individual should worry. But that assumes it is all causal!
Some on twitter argue that this study supports continued precaution taking among the triple vax’d crowd in Feb 2022. It in no way supports that. Wake up.
If I got COVID19 prior to vaccination, do I have to worry about long term CV complications compared to if I didn’t get COVID?
The study also cannot answer this question. The authors do not use a sero-prevalance denominator, so they are only showing outcomes from people sick enough to seek medical care (either for covid or other reason) and then get tested for COVID. Moreover, the study cannot separate the effect of covid from the effect of getting ensnared by the medical system. There is an old saying in medicine, “show me a healthy person, and I will show you someone who has not had enough tests.” The more you test the people who come to the hospital, the more diagnoses you will find. The control patients did not get the full force of American testing exceptionalism. Finally, there is likely residual differences between the Vets who got COVID in 2020 and those who did not that covariate adjustment/ IPW cannot capture. COVID afflicts greater toll on the vulnerable/ socioeconomically marginalized/ disadvantaged.
If I got COVID19 do I have to worry about long term CV complications any more than someone who recovered from Influenza in years prior?
This is a huge error of the paper. We know the authors have access to influenza data. I know that because they used it before in a BMJ paper. So what am I to think that they don’t use that here? I want to know if covid is WORSE for cardiovascular risk than influenza in years prior. It is highly curious that they do not provide this data. What am I to think?
How much resources do we need to set aside for helping COVID19 survivors in years to come?
The authors claim, “Second, given the large and growing number of people with COVID-19 (more than 72 million people in the United States, more than 16 million people in the United Kingdom and more than 355 million people globally), the risks and 12-month burdens of cardiovascular diseases reported here might translate into a large number of potentially affected people around the world. Governments and health systems around the world should be prepared to deal with…” etc etc.
But these results are from a US Veterans administration hospital whose population is very different than the broader national population (heavily white man & lower SES) and generalizations cannot be made to the world. End of story.
Moreover, resources need to be deployed not proportionate to the burden of disease, but proportionate to the absolute risk reduction of amelioration/ those resources. I have been trying to educate people about this for years now. Read this to learn more.
In conclusion:
I have no doubt that veterans who got a COVID diagnosis in the EMR pre vaccine have more CV diagnoses thereafter. I also have no doubt some of this is due to COVID. But some of this is also due to more testing, and some of this is that these people may be sicker to begin with. The authors fail to exclude these latter possibilities.
This study has nothing to do with people who got COVID after vaccination. It has nothing to do with Omicron. It cannot tell me if COVID is worse than the flu. PS: Why did they not do that? It does not in any way tell me that after vaccination, I should continue NPIs. It certainly does not clarify the population burden of disease, not in the USA, and not around the world.
Finally, long covid/ post covid is surely partly a real biologic event, but it is also a self fulfilling prophecy. The more we seed the literature with stories of long covid, the more we publish papers like this, the more doctors will look. The more you look, the more you find. Show me a healthy person, and I will show you someone who has not had enough tests. Investigators are highly biased as post Covid is a gold mine for research funding. The more you fund something, the more you will find it as well. It would be wonderful if medicine returned to scientific principles, ran careful studies, and had appropriate skepticism, but that medicine is dead. Covid killed it. It was patient zero.
As always I appreciate your analysis of papers that make headlines and appear to be “game changers” to people without the knowledge/training to put in proper context. I have been in medicine for 30 years. You are correct that skepticism in medicine is dead. I call todays physicians “bandwagon doctors”, always jumping to put all their patients on the latest, greatest (most expensive) medications and our medical schools are churning them out by the thousands. Bring back #conservativemedicine
Journalism is dead too in terms of providing balance. And it’s too bad that a tiny fraction of the population will get exposure to Vinay’s perspective vs. that exposed to the headlines. Goldmines proliferate, but more of them exist in the space to keep COVID top of everybody’s mind.