
Paxlovid was a 10.6 billion dollar taxpayer funded mistake
Paxlovid and Tamiflu and how history doesn't repeat itself, but rhymes

Paxlovid (Nirmatrelvir–Ritonavir) is an oral anti-covid medication made by Pfizer. The original randomized study (EPIC HR) evaluated the product in adults who had a high risk of hospitalization from COVID-19, who were unvaccinated, and who largely had not had covid before (i.e. largely, they were un-immune). EPIC HR found the drug lowered the rate of hospitalization or death (from 6.3% to 0.8%). By 2021, however, these data were obsolete, and there was a debate raging in bio-medicine.
Some physicians and researchers, myself included, felt that in order to recommend Paxlovid to younger adults, those who had been vaccinated, those who had already had covid, or both, we needed positive randomized trials to support its’ use. Others, including most famously the Biden COVID Czar Ashish Jha felt that one could extrapolate to these lower risk populations. Dr Jha spent massive tax-payer money on his faith in Paxlovid.
He frequently appeared in the media claiming that Paxlovid was underused, and pushed it widely, even outside of the EPIC HR population.
Many famous individuals who had already been vaccinated and boosted proudly took the drug. (Also from Gemini).
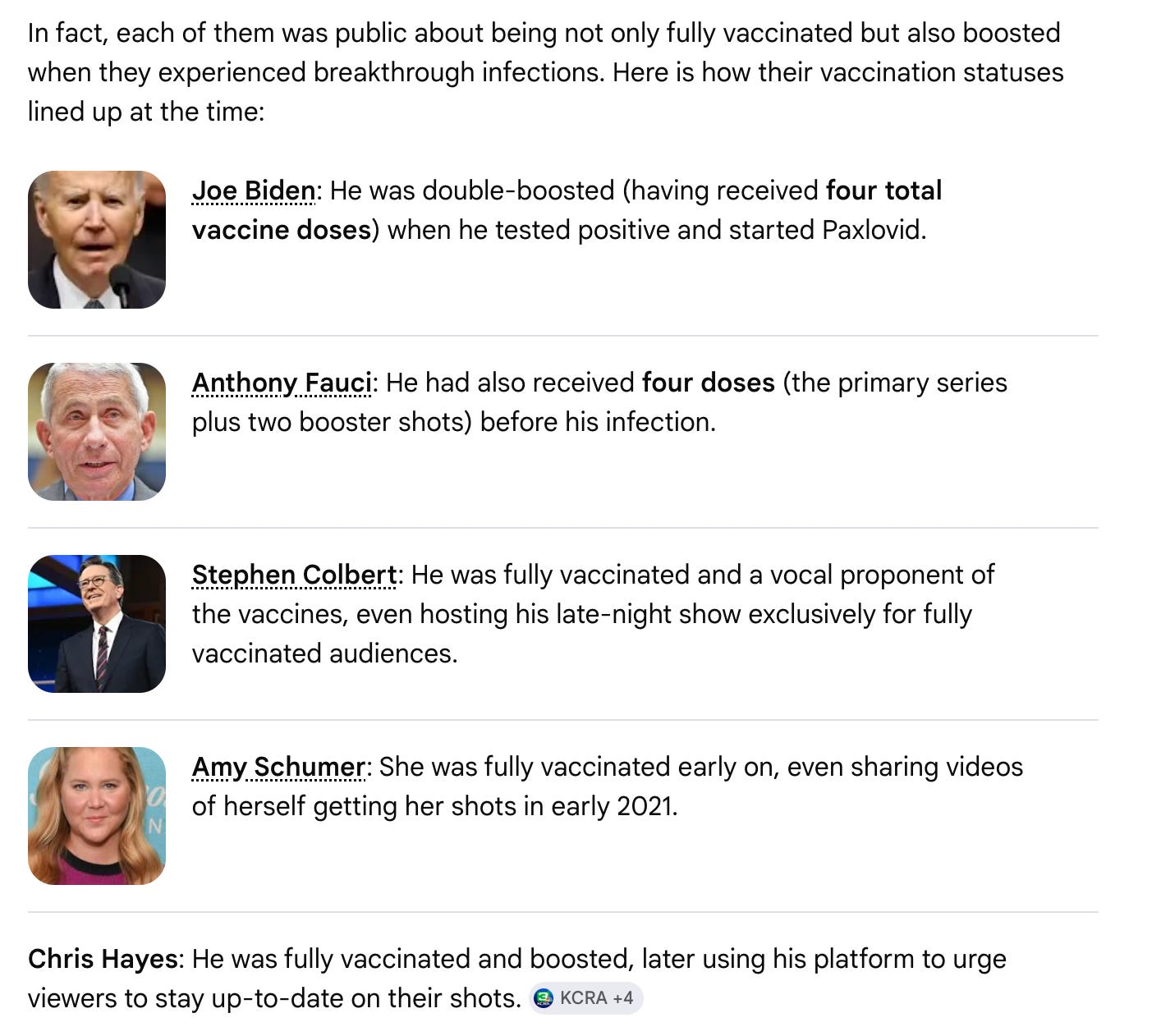
All took Paxlovid.
Meanwhile, my colleagues and I cautioned that the use of Paxlovid in populations outside of EPIC-HR without further randomized data was a gamble. A guess.
We performed a systematic review of all the randomized data, which undermined claims of efficacy.
We warned that observational studies were unreliable, and plagued by immortal time bias and residual confounding. The Biden administrations spending outpaced the evidence.
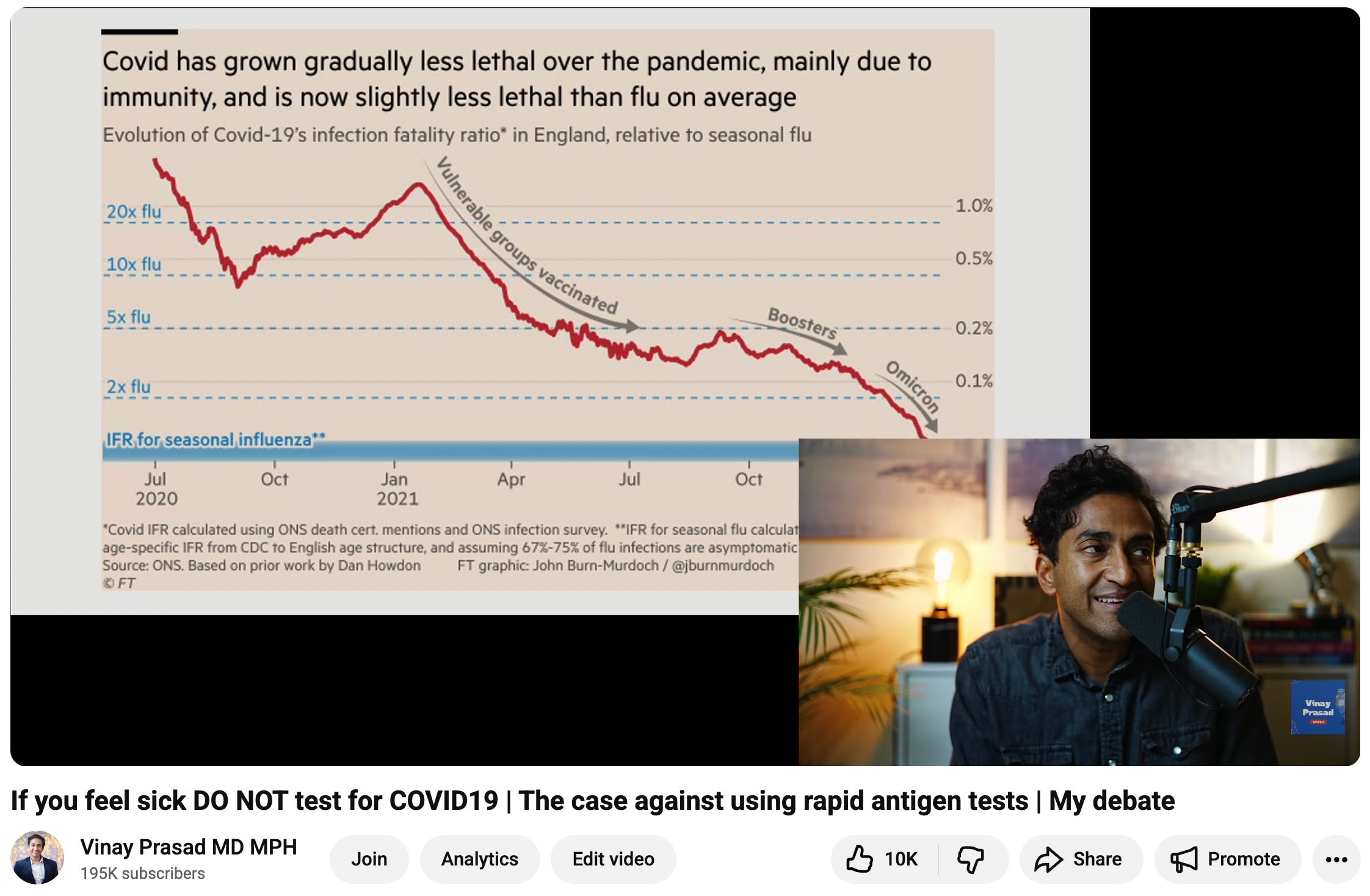
I pointed out how COVID’s declining hospitalization rate meant that EPIC HR was irrelevant data in a video on the topic, based on a UCSF presentation I gave.
Well, now the results are in:
From 2 trials— the primary endpoint is stone cold negative
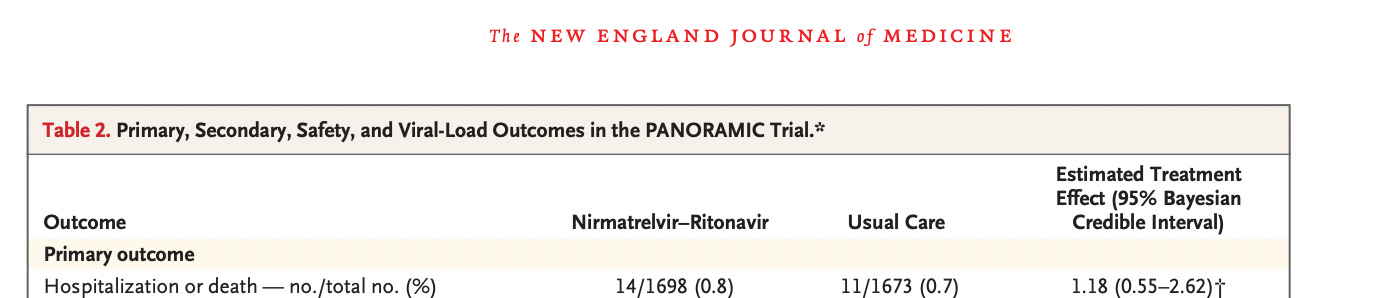
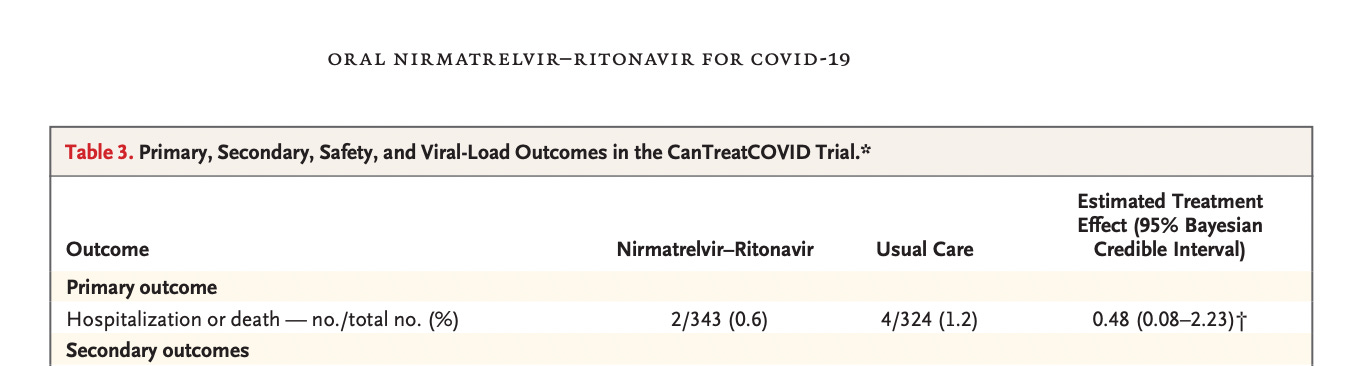
And more importantly, the event rate is so low, it would be futile to continue the study.
The authors claim improvement in some secondary endpoints like time till you recovered from symptoms but those are (a) tiny absolute differences and (b) biased and unreliable estimates. In an unblinded, open label trial people who take the pill may report feeling better due to placebo effect and a not real effect. To truly test their hypothesis, the authors should have used a placebo that contained a tiny bit of zinc or other substance to mimic the metalic taste that plagues the product. An active placebo is necessary for these endpoints. Since this was not used, the trial cannot inform symptoms. *the virologic study is uninformative as well, it could be coinicidental & not substantiating.
One final irony is that Jha favorably compared Paxlovid to Tamiflu, a drug nicknamed “Scamiflu” because it’s tiny reduction in symptoms was offset by initial toxicity, and because it didn’t improve outcomes that mattered (like hospitalization)
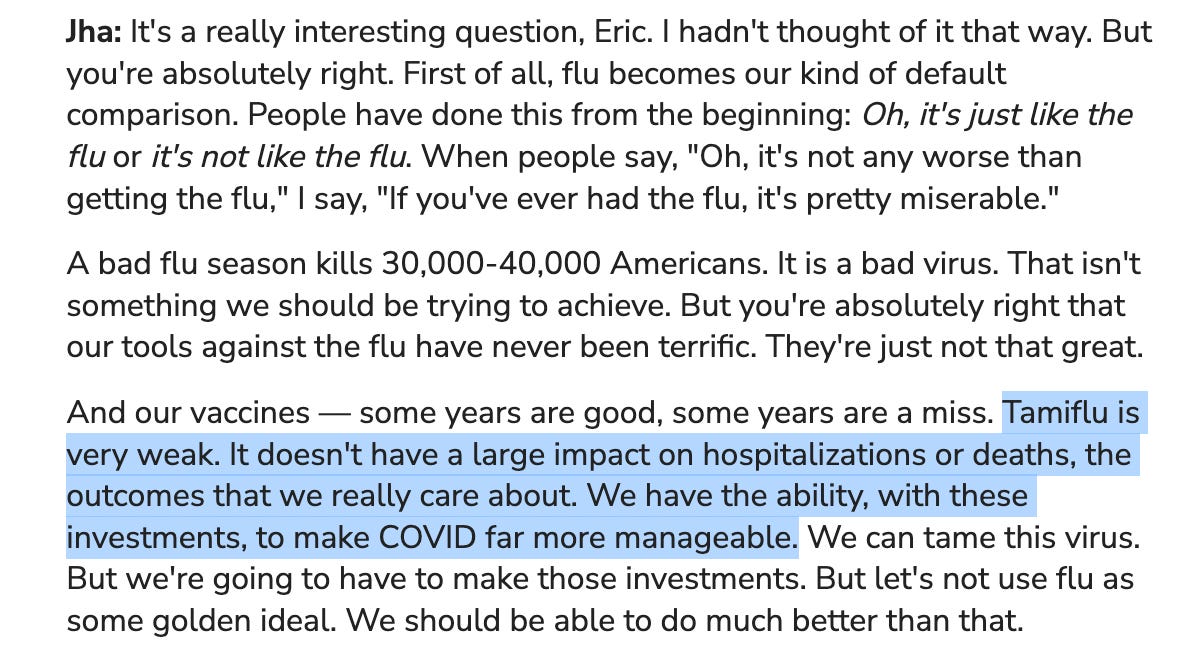
The irony of course that Paxlovid turned out to be precisely the same thing.
History doesn’t repeat itself, it rhymes.
One last thought for subscribers…
