
Progress in oncology: a tale of two graphs and two diseases

Recently a post went viral showing progression free survival over time in multiple myeloma.
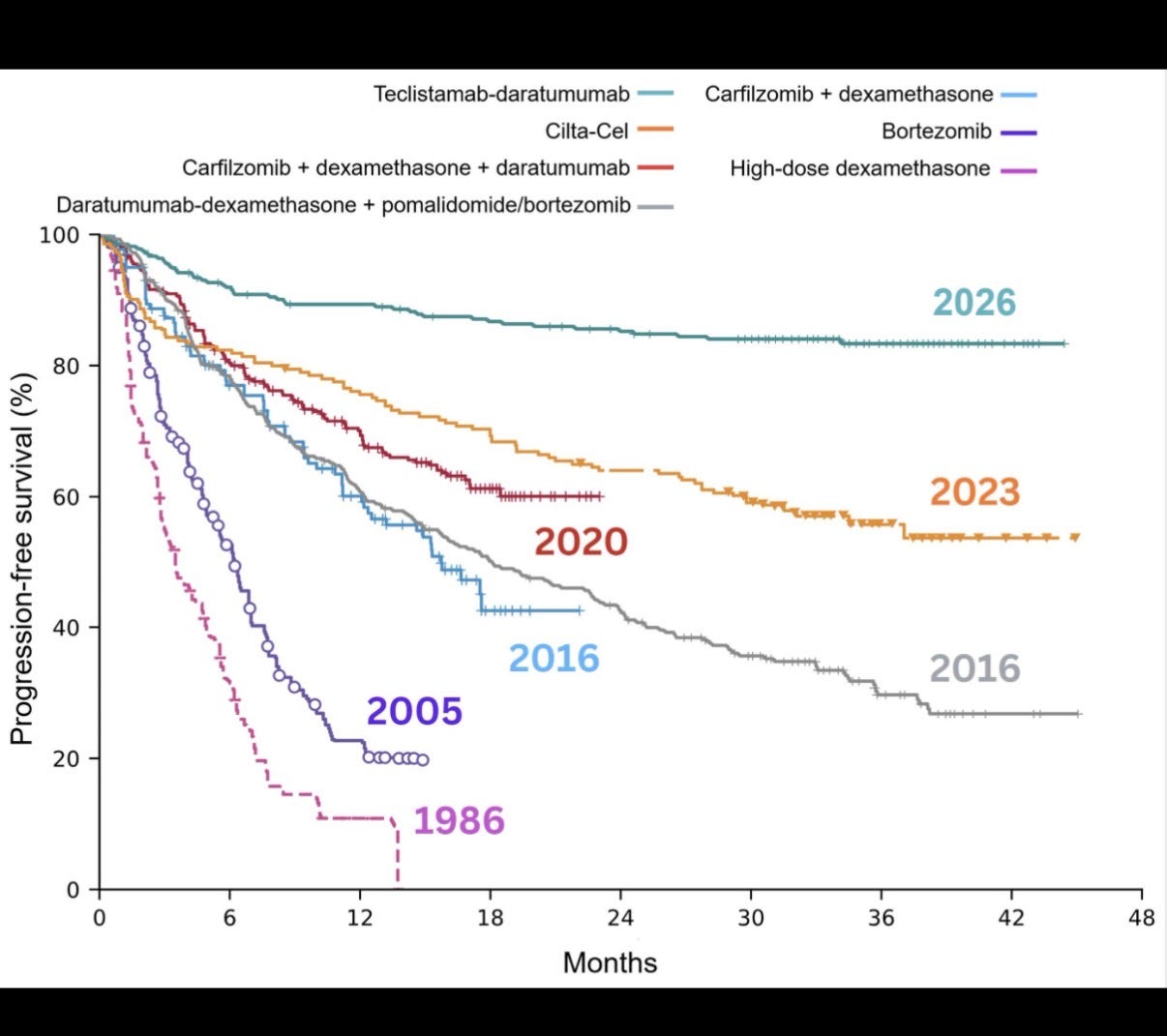
From 1986 to today, a death sentence appears to be transformed. Most of the gains happened 2005 to present. Doctors online attributed the improvement to new pharmaceuticals.
Meanwhile if you look at how many people get the disease and die of it annually (adjusting for the population age structure, i.e age adjusted) it looks like this:
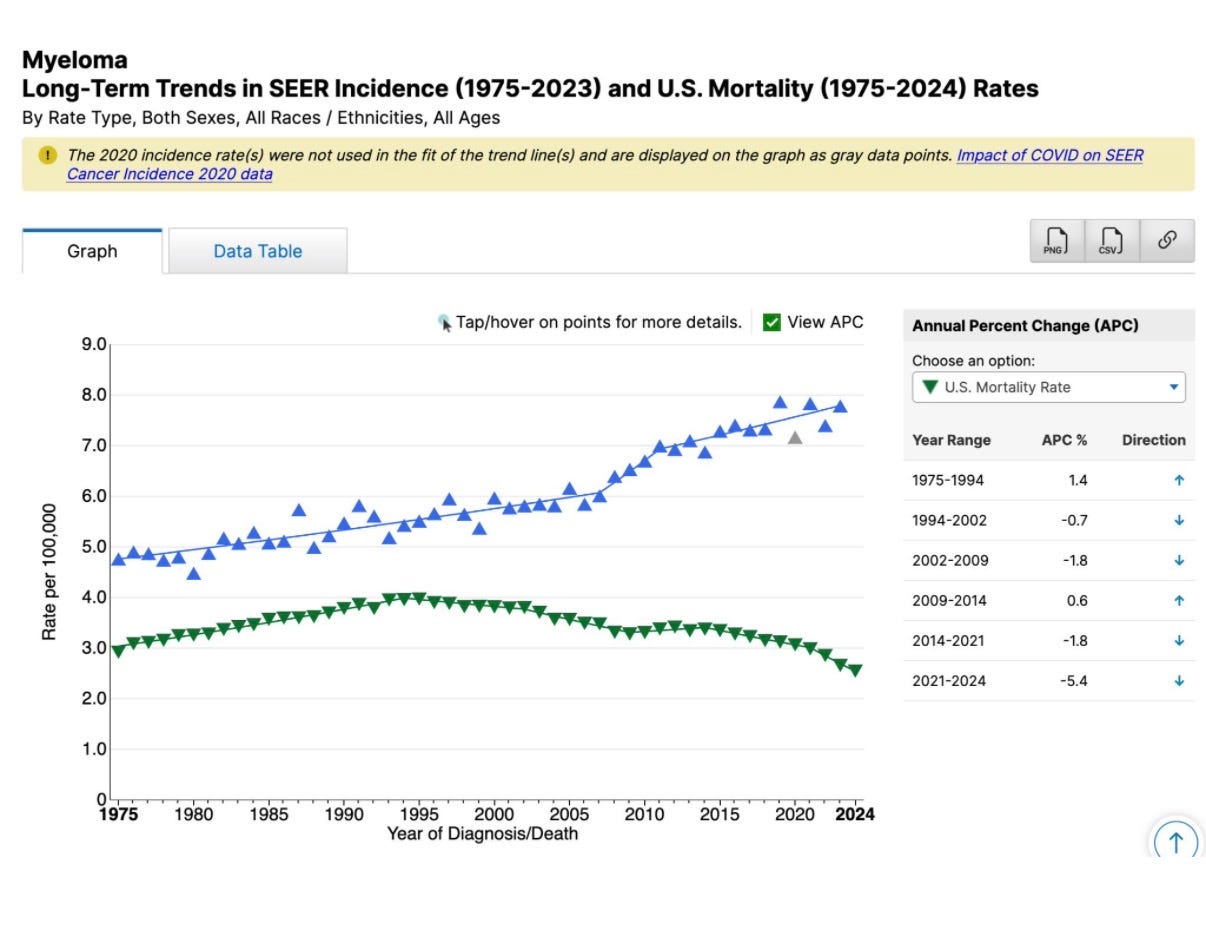
The blue line means each year more people get myeloma. And that is NOT because Americans are older, even though myeloma happens with age.
The figure adjusts for this— the graph means that more people get myeloma at the ages of 50, 60 and 70 (on balance) than ever before. From 5 to 8 per 100,000. A 60% increase.
The green line shows the death rate from myeloma, which is declining from peak levels. The graphic captures delaying death. In other words if new drugs extend life— even if all patients eventually still die of myeloma— that would mean more 64 year olds make it to 65, 55 years olds to 65, etc, and the graph would fall.
When it comes to the green line we see a modest decline. From 3 to 2.5 per 100k if you look at all times. A 16% reduction. From 4 to 2.5, if you take it from the peak, a 38% reduction (but why did it go up?)
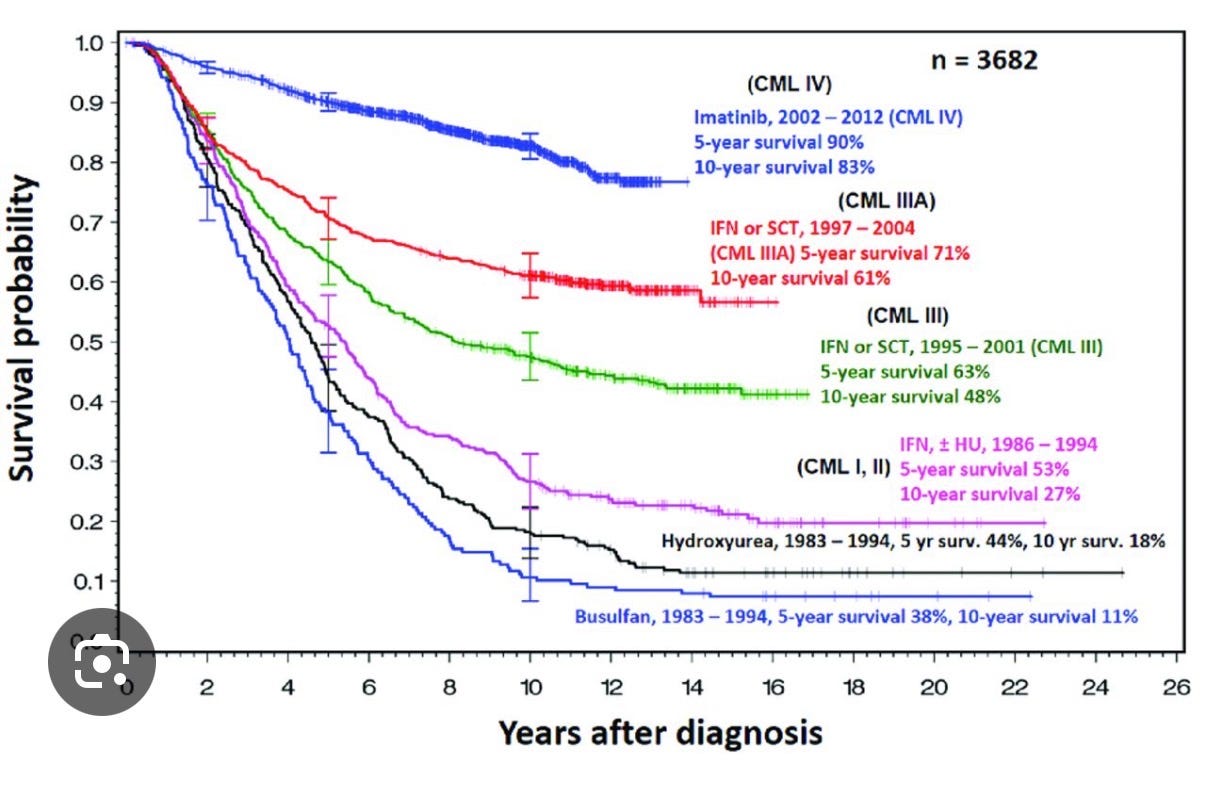
Let’s look at the same figures from CML as that represents a disease that everyone agrees is a home run.
We see the same impressive PFS curves like myeloma over the last few decades
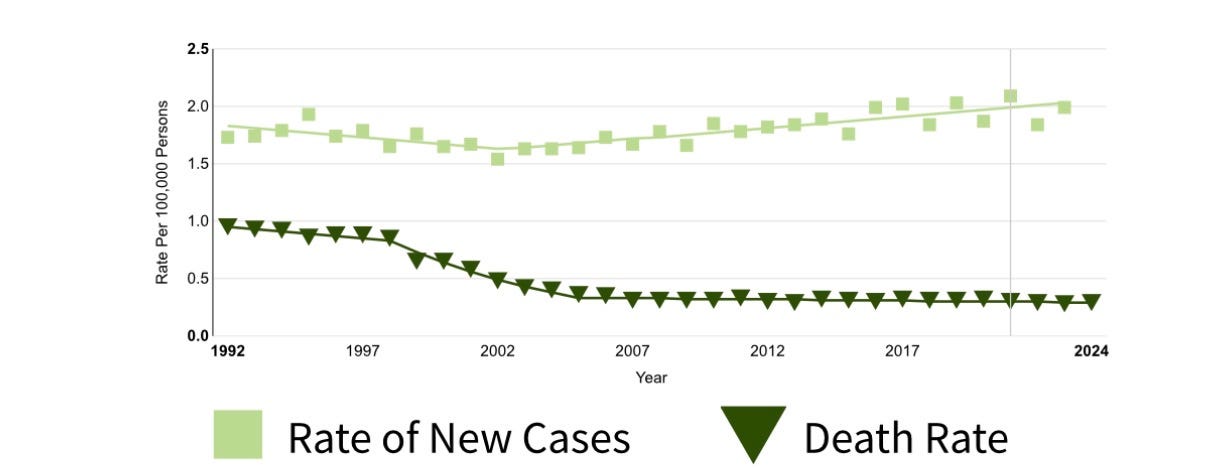
Yet incidence is more stable and death rate is more than halved. A 70-80% reduction in death rate!
Now we have two cancers, and two sets of figures.
The first figure is a tale of outcomes measured from diagnosis and the second is the population, age adjusted changes
We call outcomes from diagnosis survival and age adjusted death rates the mortality rate.
Both cancers have huge gains in the former, but different outcomes in the latter. Survival looks great for both, but CML has seen bigger gains in mortality.
What gives?
What is responsible for the reduction in deaths?
Why is myeloma incidence up while CML is stable? (Both are blood cancers)
Why does CML have a larger mortality reduction even though both have the same impressive extension in survival?
And the corollaries
—Do we just need to wait longer to see better gains in myeloma?
—are CML drugs given widely but myeloma drugs given more selectively?
Finally: Things are better in all the figures, but which is the best measure of progress?
And Bonus: why is this Substack the first you are reading about this? (You might be asking)
I will answer these questions here.
What is responsible for the gains?
The majority of the gains in CML can be attributed to just one drug imatinib, while only some of the gains in myeloma are attributable to many new drugs.
In myeloma, the major sources of gain are imids, proteosome inhibitors, cd38 abs, and bcma targeted therapy. And btw 1992-2004 auto transplant and eliminating therapeutic nihilism and giving cytotoxic chemotherapy.
Both tumors benefit from better supportive care throughout all times. Likely similarly as both are blood based tumors whose complications include infection.
Myeloma benefits more from advances in and use of radiotherapy as it can have radiosensitive lesions.
Myeloma incidence is up but cml is stable, why?
Both cancers have increased diagnoses because of more opportunistic screening. In other words, the more blood tests you run, the more you will find abnormalities that prompt diagnosis. Spoiler: docs today run more blood tests.
I suspect cml went down slightly and then up bc diagnosis shifted from white count and differential + smear to pcr for bcr abl. Incorrect diagnoses in the before period are offset by correct diagnoses (with less impressive wbc elevation) in the latter. On balance for every case you had wrongly diagnosed you pick up one rightly today. Overall things are stable.
Myeloma is way up bc of a completely different work up landscape with extensive and vigorous use of bone marrow biopsy and pet imaging. Combine this with better immunohistochemical staining, pathologists who like to up call, and you are finding way more cases. Myeloma is more subjective a diagnosis than CML as it lacks a genetic signature.
We have to also remember that the definition was changed by some doctors. Slim criteria are added, 60% plasma cells alone gets you there, etc. Changing the definition expands the incidence overnight. It also ruins the ability of survival to capture therapeutic benefit as it also captures lead time of the people diagnosed who otherwise would not be. It ruins the ability to present the first figure credibly as a scientist.
Some of increase in myeloma diagnosis means finding people who benefit from treatment who would otherwise have been missed in the past, and part of it reflects over diagnosis— finding people who don’t need therapy.
It’s worth remembering that myeloma has a massive reservoir of smoldering and mgus. Meaning many people have expansion of plasma cells that would not historically have caused discomfort or shortening of life. Some are now called myeloma.
Myeloma may yet increase when future doctors change the definition again, which I predict they will do.
Why does CML have a larger mortality reduction? (Even though both have similarly impressive survival gains)
As noted, survival is an unreliable metric of progress in myeloma because the definition has changed, and because the disease is being picked up in people whom it was otherwise ignored or missed.
The reason the mortality reduction is better in CML is because the drugs are better.
As for the corollaries: yes it is possible we will still see further gain in myeloma, but not to the extent of CML based on currently approved therapies.
It is highly unlikely that costly TKI is reaching more patients than costly myeloma therapy, but it is very likely that cml therapy works better for older people who are not included in clinical trials than myeloma therapy does. In other words CML has less efficacy-effectiveness gap— the effect of imatinib is excellent in Americans with additional medical problems, who were not in the clinical studies, whereas myeloma therapies likely have a larger gap meaning they work worse in these excludes patients.
Which is the better metric of progress?
Population age adjusted mortality rate is the correct/ only measure of progress in all diseases. This is not a new insight. It has long been known survival from diagnosis is misleading. A person can die on the same day, but you will improve survival by diagnosing them sooner. Meanwhile, mortality rate can only be affected by real increases in longevity.
Overall: There is progress in both diseases but more in CML. CML is more clearly a success story. There is much room for progress in myeloma. Myeloma is not yet curative, sadly. Presenting survival over time is misleading and masks more complicated narratives.
Why is this the first you are reading this?
