
Tracy Beth Hoeg, MD PhD: The Interview
An interview with a pro-vax, pro-kid, pro-safety, courageous physician-epidemiologist

I followed Dr. Tracy Beth Hoeg throughout the pandemic, and appreciated her analyses; Here, I let her to explain her work and philosophy in her own words. When the dust settles during this pandemic, I think more will see her as I do: pro-vax, pro-kid, pro-safety, but above all else, a courageous scientist.
-Vinay
Tell us about yourself?
I am a physician-mom, Danish-American dual citizen in rural private practice in California with an MD, PhD. I am physical medicine & rehabilitation specialist. I have also worked in epidemiological research for over a decade and, during the COVID-19 pandemic I have had multiple studies related to children published in major medical journals. I have ongoing studies or pending publications looking at masks in schools, school-based COVID-19 screening testing, boosters in children, risk-benefit calculations of the first and second dose of mRNA vaccination in children and a case series of booster-associated myocarditis. Unrelated to COVID-19, I’m working on randomized trial of treatment of acute ACL tears with UC Davis, a study on arrhythmias in ultramarathon runners with Oxford and a large bone health study with Stanford.
You are someone who cares about balancing the efficacy of vaccines and minimizing their harms—is this an accurate characterization?
Absolutely. My interpretation of the data is vaccines continue to be the best tool we have to prevent severe disease. When health care workers could get vaccinated, I got mine the first day I could. That being said, I had wished my parents and older patients could have gotten theirs before me. I begged unsuccessfully to extend my time between the first and second dose because of cardiac side effects I had had from the first dose (which came on quite severely while running). I continue to strongly recommend vaccines to my patients (and now boosters for all over 40-50 or with specific risk factors) and help facilitate vaccination appointments for them and talk them through the data.
I recommended to my younger healthier adult patients to only get one dose if they had already been infected based on the data we already had late last winter and a need to preserve vaccinations. I have always felt, based on the data that healthy children were at very low risk and vaccinating them before older adults across the world was unethical and irresponsible. You and I wrote about this for the Atlantic with Monica Gandhi. I still stand by what we said.
Over the spring and summer, the evidence suggested vaccines were very effectively preventing transmission, which was a major rationale for vaccinating everyone. But I also knew, as did you, in the spring that a serious vaccine adverse effect could quickly tip the individual harms of the vaccine beyond those of the benefits for healthy children. And I actually tweeted about the uncertainty about the risk-benefit ratio of vaccination in healthy boys on June 10th as the myocarditis data were accumulating from Israel and our own CDC.
My tweet was censored by Twitter and that landed me on Tucker Carlson (which I had never watched). I understand the political nature of this pandemic (certainly on social media) but the censorship of an issue as important as vaccine-associated myocarditis in boys and young men really got under my skin. I was receiving texts and messages from physicians I knew seeing post-vaccination myocarditis in young boys and men across the country and I was vexed the CDC did not prioritize getting an accurate, stratified estimate of this occurrence. Certainly, as a mom I wanted to have a reasonable sense of the benefits vs risks in my old children. At that time I was glad to connect with the cardiologist John Mandrola because we are very like-minded, particularly on this issue (we’ll discuss our study below).
I have consistently viewed attempts to estimate the rates and define the severity of a vaccine side effect as highly pro-vaccine. Anything else, especially when it comes to children, will quickly erode public trust and fuel overall vaccine hesitancy. Especially now with the vaccines’ limited and transient impact on transmission, we need to be considering each individual’s risks from COVID-19 and their expected benefits (and risks) from each dose. The most important factors to consider in this analysis include age, sex, risk factors for severe COVID-19 and history of infection.
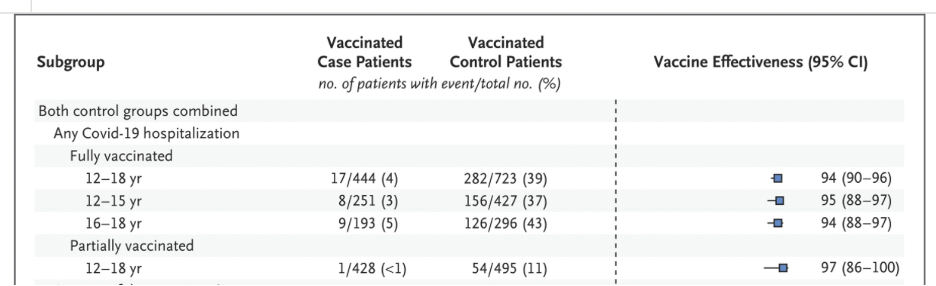
What still boggles my mind, is when you just do the simple math using the German study of infection-hospitalization rates in healthy children, you get a 1/2400 chance a healthy 12-17 year old will be hospitalized for COVID-19 requiring specific covid treatment (this eliminates incidental hospitalizations) and, now with omicron, that is likely around 1/5000 risk (or lower) and yet the rate of symptomatic post vax myocarditis after dose 2 in this age group is around 1/3000 (see below) and yet so few seem to be questioning dose 2 for them (when mathematically it’s the wrong decision), let alone dose 3, which seems a clear mistake to mandate without evidence of benefit. And the most recent NEJM study of vaccines in children found dose 1 may actually alone have all of the benefit in terms preventing hospitalizations (see Figure 2, which is shown below). These are important details that should be used to minimize harm.
You co-authored a preprint estimating the risk of myocarditis in young men. I am wondering if you could summarize your findings?
Yes. John Mandrola, Alli Krug, Josh Stevens and I did a thorough analysis of the VAERS database at the end of June of 2021 and found rates of myo/pericarditis of 162 and 94/million in boys 12-15 and 16-17 after dose two. The most unique thing about our study was we included a risk-benefit-analysis which took health status and disease prevalence into account, and we found that the risk of myocarditis after dose 2 in healthy boys 12-17 exceed that of their hospitalization risk for COVID-19 over a 120-day period even at times of high disease prevalence. We also found a high post-vaccination myocarditis hospitalization rate of 86%, though this was lower than the >90% reported by the CDC. We found post-vaccination myocarditis occurred at a median of 2 days after vaccination and was around 7x more likely to occur after the second dose than the first and occurred about 9x more frequently in boys than girls.
Your estimate of myocarditis was 162 per million and 94 per million for boys aged 12-15 and boys aged 16-17 respectively. Can you contextualize this estimate and compare it to other sources? Were you an outlier?
Our identified rates were around 2-fold higher than those reported by the CDC. In the below figure in orange you can see how the rates we identified stack up against other post-vaccination myocarditis rate estimates in this age group stratified by dose number and sex. As you can see our estimates have not ended up being outliers. I think this speaks to the utility of the VAERS database for beginning to estimate rates of a condition. Indeed, our estimate appears to be an underestimate looking at data from Hong Kong and Kaiser Permanente Northwest (as expected due to underreporting in VAERS). At the time of our preprint only the Optum and CDC rates were available (beyond the initial Israeli rates)

Figure by Alli Krug, Josh Stevenson and Tracy Beth Høeg
Many probably remember the CDC was initially consistently reporting a rate of 1/80,000 for 12–39-year-olds for post vaccination myocarditis all the while knowing the rates among young males were the highest and not separating that group out. I know you were very quick to point out the risk to young women from VITT from the J&J vaccine and, for some reason, this was less controversial. I also wrote at that time it would be unethical to do the J&J vaccine trial in girls <18 for this reason and I am glad it was not run. I have to admit it was unexpected that when our research group stratified reviewed the applicable VAERS cases that we were attacked for releasing what was then and is now a reasonable (though low) estimate. Myocarditis is not always benign and three different reports have indicated about 80% of post vax myo cases have late gadolinium enhancement on cardiac MRI which may be associated with arrhythmias later in life. There have also been 3 confirmed deaths I am aware of (one reported in NEJM) and one under investigation by the CDC.
Some alleged that you used the VAERS system improperly. My understanding is that a cardiologist reviewed all putative cases of myocarditis— and confirmed they were highly likely to be related—in which case, your use would be proper. What are your thoughts?
VAERS is a passive surveillance database that was created for vaccination safety signal detection such as new or rare adverse events and particularly to assess the safety of newly licensed vaccines. We (yes, including a cardiologist, John Mandrola) went through all entries to ensure there was objective evidence of cardiac damage and that these were not self-reports of just "chest pain" but required the same objective evidence of cardiac injury that the CDC did in their analysis and excluded many potential cases of real post-vaccination myocarditis if we were at all in doubt. VAERS has historically been used to identify multiple vaccine-related safety signals as discussed here. It should also be said that the NEJM reviewed our study (though obviously did not end up publishing it) but we incorporated their very helpful suggested changes and the study was also reviewed by additional highly respected physicians and epidemiologists who need to remain unnamed, but reassured us our methods were appropriate. All of this made it easier for me to see that, while there were some appropriate critiques of our preprint, most of the allegations about our methods being improper seemed like people simply jumping on the bandwagon because they thought it was virtuous to fight what was they incorrectly perceived as anti-vaccination propaganda.
But as to whether or not these myocarditis cases were related to the vaccines, 1) as you can see below, most cases occurred a median of 2 days after vaccination 2) if one looks at the appropriate expected background rate of myocarditis in boys of this age, it’s about 2/million/week. Because most of our cases occurred within a week of vaccination our rates of 162 and 94 per million were clearly above the expected background rate. 3) we eliminated all cases in which the VAERS entry indicated other cause (such as viral) could not be ruled out. Given proximity to the vaccination, our strict case inclusion criteria and greatly exceeding the expected background rate of myocarditis, I don’t doubt these were true myo/pericarditis cases related to the vaccine. One can not be 100% sure about all of the cases, but clearly the signal is there even if there continues to be some uncertainty about exactly how common it is.

Høeg et al. https://www.medrxiv.org/content/10.1101/2021.12.21.21268209v1.full-text
A new preprint by Katie Sharff suggests the CDC’s method of tabulating myocarditis is inadequate. Can you explain this paper and its results?
Yes, this was a very impressive study undertaken by Dr. Sharff and colleagues and reading this paper really made me want to meet Dr. Sharff because she must be really cool. They performed an extensive medical record review of over 150,000 patients 12-39 within the Kaiser Permanente Northwest System and identified rates of 1/2700 and 1/1900 males 12-17 and 18-24, respectively, after the 2nd dose. First, that was interesting enough and the 1/2700 was consistent with the rate of myocarditis in 12-17 year olds already identified in Hong Kong after dose 2 but second, it raised the issue (though they didn’t mention it in the paper) of the higher rate in the 18-24 year olds possibly being related to Moderna use in those 18 and older (I still can’t believe the US has not curtailed the use of Moderna for males <30 as much of Europe has done, but that is an aside). The other major finding of their work was that the vaccine safety datalink (VSD) would have been unlikely to identify the majority of these cases, at least not in a timely manner, without the extensive chart review that they performed. The vaccine safety datalink is one of the ways the CDC monitors for adverse vaccine reactions and includes nine healthcare organizations.
Have you been surprised by the personal attacks you received regarding vaccine policy? If so, in what way? Why do you think this topic is a third rail?
I wasn’t really surprised by the attacks. I had gotten used to attacks after writing and publishing about misunderstandings about COVID-19 risks to children, challenging school and sports closures even in the summer of 2020 and pointing to the lack of data supporting masking in schools. It’s fairly easy for me to separate out people who are coming with new data or useful debate from those who want to prove a point by making me out to be a bad person. The former I value greatly, and the latter is just such a waste of time. I guess my surprise has come in the form of disappointment in people chose to squander their limited time on attacks when they could be contributing to the discussion. Why third rail? First because the stakes are high both in the form of COVID hospitalizations and death and the idea of heart damage to children. But there is also a laser focus on COVID-19 policies in social media right now in the form of (“what team are you on?”) and it’s toxic. Debates about this topic should be happening at universities and not on Twitter and yet, here we are.
Let’s turn to masking: What are your views on compulsory masking in schools and day care?
Data supporting cloth masking has just never been there. I’m old enough to remember the beginning of the pandemic when physicians were outraged, they didn’t have access to properly fitting N95’s. I remember putting a buff over my face in Target in February of 2020 and realizing I was a lunatic because there was no way it was protecting me. The two randomized controlled trials we have now on cloth masking (DANMASK and Bangladesh) found no effect of cloth masks and, as Maria Chikina, Ben Recht and Wes Pegdon nicely showed, by most analyses, even the surgical masks would not have been found to have had a significant impact on cases from the Bangladesh study. Certainly, the study found no impact of surgical masking on anyone under 50, which is continuously overlooked (if they did find even a minimal effect it’s a highly debatable one considering the effect they found was in the context of increased distancing and education about COVID-19 in the masked group. Really that study randomized many interventions which may have worked, not just masks).
In terms of the effects on masking children in schools, beyond the multiple studies we have showing no correlation between student masking and school cases (including one by the CDC from Georgia), all one needed to do was look at Scandinavia where they never masked children <12. In fact, at the same time as our Wood County Wisconsin study (finding minimal spread in the schools with around 90% masking compliance), there was a study done in Norway that found similarly very low rates of in school transmission (“minimal”) where students were not masked. Beyond this, Scandinavians have been much better at acknowledging the downsides of masking. My friends and family in Denmark and Sweden have been appalled our young children have had to wear masks in school (even my very pro lockdown Swedish friend (this is actually not an oxymoron) was surprised the US was masking young children). There are clear downsides for children with hearing and speech problems, not to mention the constant reminder that they must look at each other as vectors of a dangerous disease. We’ve suffered from the illogical type of thinking that if we don’t hear children complain that means they aren’t suffering. That makes me sad. Though I, like many people, accepted masking children in the beginning of the pandemic simply so they could attend in-person school, I view continued compulsory masking of children to be unethical given the lack of evidence of benefit.
I have written more on this topic for the Canadian National Post with Pooya Kazemi, Jennifer Grant and Martha Fulford.
I’m including here preliminary data from a study I am part of with two paired school districts in the same community (both K-12, both with around 12,000 students, very similar demographics, 2% higher staff vax rate in the school with the mask mandate) showing no obvious correlation between the student case rates and masking policies. FPS has (blue) has a mask mandate and WF (yellow) has masks optional. The FPS (blue) district will be going masks optional this week so we will start a partial crossover period in our study. This study has further influenced how I view school-based mask mandates.
Blue- Fargo Public Schools (mask mandate)
Yellow- West Fargo (masks optional)

Data from Neeraj Sood, Shannon Heich, Josh Stevenson and Tracy Beth Høeg
What do you think about the fact that the CDC and AAP (American Academy of Pediatrics) recommending kids as young as 2 mask for the entire day?
Age two is really the critical period of language development. Robert Hughes, Sunil Bhopal and Mark Tomlinson have written eloquently about this. You had a very nice interview with Rob and Mark, who are true experts on this topic, and they were strongly opposed to masking children at this age because of concerns about its effect on their development. Furthermore, children of this age cannot and should not be expected to properly wear a mask. I worry about abstract things like their sense of feeling trapped or their development of interpersonal skills. It should give the AAP and CDC pause that the WHO and European CDC have explicitly stated children <6 should not be masking, yet it hasn’t. I like many parents I think have lost some trust in the AAP and CDC for not even acknowledging the downsides of masking this age group. Repeatedly putting out statements about there not being any valid concerns about masking toddlers I think is something many parents have found condescending and irrational.
What do you think about schools like Berkeley, California with high rates of vaccination, which have escalated masking to n95?
It’s inappropriate and lacks compassion. We are at (and past) a point in the pandemic where the appropriate thing to do is return to normal. Everyone ages 5 and above has access to vaccines effective at preventing severe disease and omicron is a milder variant than delta. My understanding is N95s are not designed for use by children. Well fitted N95s are also uncomfortable and it is cruel to force a child to wear one all day during school. I would love to see a nationwide poll of public opinion on this. I think by far most people are opposed to N95s being compulsory for children. I also suspect more physicians would be standing up against this if they weren’t fearful of losing their job or license or some sort of retaliation.
You have European connections, I might ask you to compare and contrast the US pandemic response to Europe, particularly areas that were different and you feel one continent did better.
Europe in general did much better than the United States aided by their robust pre-existing public health infrastructure and trust in their public health agencies. Europe provided paid sick leave, access to free testing for all (when available), gave transparent useful information rather than fear-based media coverage and early on acknowledged the harms associated with school closures. There was more of a societal commitment to keeping schools open as much as possible and prioritizing children’s needs over adults, whereas it was the opposite in the US. I know in Scandinavia, even during periods of school closures, free or supplemented daycare was provided for children of essential workers. Children have to be cared for while their parents are at work. Grandparents may not be available nor are they necessarily the ideal population to have given increased exposure to (pre-vaccine, especially). In the US, there were far too many underprivileged or even middle-privileged children who fell through the cracks of the system because those making the rules in our country seemed to be out of touch with the realities children and their parents were facing. Europe handled this issue better.
Were there any COVID policy issues that the US got better?
I would point out the US was successful in operation warp speed (despite the fact I would not have chosen that name!) and was very fast in its rollout of vaccines and that quick deployment of vaccines which are highly effective at preventing severe disease actually should have returned our lives to normal faster than Europe.
I also think the US has put out some of the most important scientific publications of the pandemic and that our outstanding medical education system and talented, hardworking physicians, nurses and other healthcare workers have tirelessly helped pull us through this pandemic with grace and humility. Americans who work in health care are some of the most hardworking and humble people I know, and this absolutely deserves recognition.
You are someone who has worked on many important school studies, including an analysis from Wisconsin. I am wondering if you could describe those results?
On January 26th, 2021, the study “COVID-19 Cases and Transmission in 17 K–12 Schools — Wood County, Wisconsin, August 31–November 29, 2020” was published in MMWR and I was the senior author on this study. I was actually told last week by an NPR interviewer that our study is the most-cited study on COVID-19 in schools over the entire pandemic. That really made me happy because I knew as soon as we started analyzing the results that the findings of our study had major and worldwide implications for policies around school reopening. We found that, even at times of very high COVID-19 community transmission, despite 191 cases of COVID-19 being identified within the schools that only 7 (seven) of them were the result of in-school transmission (so >95% came from the community). I remember spending hours and hours and hours working on this writeup up with Dr. Amy Falk feeling like we had a made a great discovery (children are not efficient transmitters of COVID-19 in schools; of course Europe pretty much already knew this) and we were reframing the way we should discuss COVID in schools. Rather than schools being centers of super-spreading as many had feared, we found 37% lower rates of covid in the schools than the community and no transmission to teachers. Our distancing policies varied, and children ate lunch indoors unmasked and went to recess unmasked and more details about the specific mitigation strategies can be found here. Regarding masking, knowing what I knew at the time about the Scandinavian masking policies, I was very skeptical what we found had much if anything to do with the masks. Indeed our study did not look at masked vs unmasked students. Right before publication I actually insisted we not call the study “Mask Up” as it had originally been titled and all the authors thankfully agreed. Yet to this day, it is still, for totally illogical reasons, used as a study to justify masking children in school. It also did not result in the prompt reopening of public schools that I had hoped for- and naively expected- in the US last spring.
How did you feel when those results (presented in 2020) failed to result in massive school reopening?
I was both angry and disappointed. The initial reception to our study from people like Tony Fauci, Sanjay Gupta and Paul Offit was so positive. They all publicly advocated for rapid school reopening when the findings were released along with a very similar study from Duke University in Pediatrics. They were all publicly acknowledging the tradeoffs of not reopening schools! But when the CDC came out with its renewed school reopening guidelines on February 12th, I remember being on the phone with Bo Erikson at CBS- and we listened to the CDC press conference- and I was just flabbergasted the CDC was going to be requiring stricter metrics to reopen schools. It was completely illogical and when I spoke with fellow researchers and pediatricians across the country (many of whom I know I still cannot name) we all asked the important question – who or what did the CDC get these guidelines from? It’s an important question and, it turns out, it was most likely from the teachers’ unions as the NY Post exposed here and as was also covered in Undark. And that the teachers’ unions (and I am a supporter of unions as long as there are unions for all or most trade and one does not have disproportionate power) had critical influence over the school reopening policies above that of the scientists studying this, not to mention students and parents. This pandemic has been a coming to terms for me with the fact the CDC is much more a political than scientific agency; I would love to see that change.
How bad will the damage from school closures be?
We are already seeing the rapid deterioration of the overall health and well-being of children, particularly the socioeconomically disadvantaged in the forms of depression, anxiety, weight gain and widening learning gaps. I covered a lot of this in my congressional testimony. I would never blame this all on school closures though. Correlation of course does not mean causation and parents losing their jobs, children having their access to sports suddenly cut off, increasing substance abuse, etc, I suspect have all contributed to multiple parallel public health crises in our youth. I think most people in medicine and public health saw this coming from a mile away and felt powerless in fighting it. Beyond this, we are teaching a generation of children to view each other as disease vectors and that adults’ needs are more important than theirs and that, when it comes to “protecting” them from covid, we are indirectly teaching them it is better to rely on magical thinking (like “masks work”) than to actually do and/or adhere to relevant and well-done studies. But I am an optimist and believe we Americans still have it in us to do the right thing and not repeat the same mistakes in the future.
What do you think about the main-stream media coverage of schools?
American media coverage of school closures has overall been harmful. The very first example I saw of this in Sacramento set the tone for the entire pandemic. There was a teacher at our son’s school who contracted COVID-19 very early on in the pandemic (early March) and very sadly ended up dying. The coverage of her case continued to stress that she was a teacher at X school and suggested she had caught it at school but it was many weeks later that I saw a small blurb in our local online paper stating she had actually contracted it at church and the family wanted the community to know. But that spring and the following fall, over and over, it was written that a teacher at such and such school caught covid-19 and died but for every single one of these cases (I think I stopped looking after about 20), it was eventually revealed the teacher caught the virus outside of school. But the tone of fear had been set and it seemed more and more journalists found it virtuous to make people so afraid of schools and so afraid of sending their children to schools that they would view school closures as necessary. Denmark, I must say (I read their papers and watch the news from there often), has done a great job of covering happy maskless children in school and stressing the importance of society prioritizing a normal childhood. It’s really beautiful.
I, along with Leslie Bienen and Eric Happel, talked quite a bit about the media’s distortion of data in this Persuasion article. If I had to pick one media outlet, I would have to say the New York Times has been the most egregious in exaggerating COVID risks to children and titrating to desired societal effect. Though that makes me respect the journalists there like David Leonhardt all the more who have successfully put covid-19 risks to children into perspective and in the context of the many greater risks they face.
Pre-covid what was your politics, and post covid what will they be? What accounts for any change(s)?
My entire adulthood I have sought to maintain a philosophical framework that was independent of the American bipartisan system and based on what I view as the optimal roles of the government. Especially after living and working in France and Denmark, I think of the government as being responsible for providing services, particularly that protect the most vulnerable such as universal access to healthcare and school. There are many other types of protection such as safe bike lanes and transportation and the promotion of and easy access to a healthy lifestyle with preservation of green spaces and these for me all fall under the “Big Mother” role the government should fill. On the other hand, maintaining individual liberty and freedom is absolutely critical in any healthy society. This can be in the form of religion or bodily autonomy or privacy or individual decision making. Infringing on these is what one could call the “Big Brother” type of government. I will say that Scandinavians in general tend to believe in Big Mother and are skeptical of Big Brother. We saw a very interesting example with this with Sweden where they decided lockdowns were unconstitutional. During the initial surge, I disagreed with their decision and agreed with Denmark and Norway who had a temporary lockdown and Sweden did have more deaths during the first wave. But, after that, I have strongly supported Sweden because they have been very good at acknowledging one should not have rules or mandates that disproportionately hurt the less privileged especially if they are of questionable benefit. Here in California, there has been a lot of the “rules for thee but not for me” mentality. If business lockdowns only affect the lower and middle classes but the people instigating the lockdowns do not lose their jobs, that’s a problem. This was the same for public school closures; the ruling class could put their children in private schools so their families were not suffering. I also think censorship of only one type of thinking (which I call the balanced mentality: “there are other problems besides covid” and “let’s be realistic about who is at most risk from covid”) has gone too far in the US. Also mandating vaccines in the young without clear evidence of benefit to the individual or society and mandating masks, again without good evidence of benefit are both examples of unethical government overreach. And I think the more a government a government slips towards authoritarianism, the less they can be trusted to use money wisely and properly in their Big Mother role of protecting the vulnerable. Along these lines, CDC has recently been publishing studies which tend to only show the results they want in order to get desired behavior change. So my foundational political philosophies have not changed during the pandemic but the US’s tendency towards political rather than scientific recommendations and unscientific infringement on individual freedoms has grown. This creep towards authoritarianism can quickly erode trust in any society.
I have heard that some physician mom Facebook groups have been particularly upset with you. Is this claim true? If so, why do you think that is the case, and what would you say to them?
Well, I think a few vocal physicians there did not know me or my intentions. I have been part of the Physicians Moms Group on Facebook for a very long time and I have learned so much from those ladies and had many good laughs. But the groupthink over there has become a strong and at times negative force. After I had published multiple op-eds with Monica Gandhi on reopening schools and then, in the spring about returning schools to normal – masks off – I was pretty viciously attacked. I never would have noticed except a friend alerted me to it. So I did what I always do which is start posting studies, in this case about the lack of correlation between student masking and school case counts, assuming they would be interested. I think some were but the loudest ones basically just started bullying me. I did call them out on it but it didn’t seem to work. My friends from my medical training who very kindly tried to stick up for me were quickly bullied too (always something along the lines of “you’re not taking the pandemic seriously” or “this is a pandemic we need to do everything”) and so, rather than having a productive conversation, most just backed down and stayed quiet. I’ve never been interested in fighting with people online (or offline), so I just stopped paying attention to it, but when some of them started visiting and commenting on my profile page posts and I knew my parents and relatives would be able to see, I just stopped using Facebook. That’s how silencing happens. The saddest part is, I think most moms on there wanted to have a real evidence-based conversation, but on social media there is something about the loudest most accusatory people (who are generally assuming bad intentions in others) that get the most power and attention. That’s pretty destructive.
What do you think will happen to public health going forward? Will it retain credibility?
This is such a great question and I first want to back up and state where I think we are right now, which is a place where many smart, educated Americans have lost faith in the CDC. The CDC has put out study after study this past fall on masking and natural immunity and vaccination-related myocarditis and, more recently the diabetes in children study that, best case scenario, were just sub-optimally designed and didn’t have critical enough peer reviewers or, worst case scenario were cherry picked data and/or studies simply used as a type of propaganda to get Americans to behave in a certain way. Either way, it’s problematic to have a public health agency we can’t count on to properly evaluate data or publish important studies regardless of the findings. Simply put, they need to be an unbiased, transparent, evidence-based agency if they want to maintain the trust of the American people and have their guidelines adhered to.
As one of my favorite people on Twitter, Jeffrey Flier, former dean of Harvard Medical School wrote, “As a long-standing diabetes researcher, I join my Harvard Public Health colleague in calling out the severe flaws in this CDC report claiming COVID increases diabetes risk in kids. Would never pass peer review in this form. CDC must do better.”
Yes, the CDC must do better.
But what will happen? The COVID-19 pandemic has taught me to not predict anything, but it is absolutely foundational to any society that the central public health agency is trustworthy, compassionate and diligent. I wonder if so many people are turning to podcasters like Joe Rogan for health and science advice because of issues of trust with the CDC. That is really the question we should be asking as a society is not whether or not he should be censored but why people are looking to him above the CDC and their own physicians for advice. This is actually a deeply important question and I say this with Denmark in mind, where there is incredible trust in the Sundhedsstyrelsen (the central public health agency) and this has been critical during the pandemic and will continue to be far beyond.
Do you think checks or balances need to be placed on the ability for Governors to declare a health emergency? Why or why not?
Well, again, yes. I agree with what Sweden did during the pandemic past the initial couple of months by valuing individual freedoms and human rights. It resulted in less collateral damage especially to the economically disadvantaged and the most vulnerable in their society. And though I disagreed with them not having an initial lockdown, which resulted in higher COVID-19 mortality than Denmark and Norway (which are culturally, geographically and linguistically very similar) they are one of the countries that ended up managing the pandemic the best. We also cannot have a situation, as we have had in the US, where the difficult rules only result in harm to the lower and middle class and the upper class is unaffected. That is really a dangerous type of authoritarianism and results in further wealth and health disparity. You have mentioned it many times, but the taking away of the freedom to go to a park or run out on trails is something I never thought I would see in the United States. I actually wrote about the serious collateral damage (for no appreciable gain) from shutting down outdoor racing events here last fall. Furthermore, I never thought I would see 2-year-olds or children with other disabilities forced to wear masks for hours a day (as a physician mom who spent 9 months of my residency at UC Davis working in pediatric rehabilitation and as a former teacher of special needs children in France, I feel like I have at least some of the qualifications to be able to opine on this). But in summary, of course there needs to be a limit to the rules a governor or government puts on their people, especially if they themselves are immune to the downsides of those rules.
Anything I missed?
Yes! You have been an incredible resource during this pandemic and someone many people look up to for your reasonable and insightful takes on the ever-changing sometimes mind-boggling policies we are facing. I could hardly believe my ears when I heard you being interviewed on Z-Dogg last fall and I thought, wow, another physician actually gets it; you were one of the first to emerge as a rational voice at that time. So, thank you for all the work you have put into your writing and interviews. I have learned an enormous amount from you and your guests. And actually, that is what I think of when I think of the future of public health: people coming together to have uncensored discussions using data and team work to put forth reasonable and compassionate policy recommendations.
More about Tracy Beth Hoeg, MD PhD…
I see patients of all ages with pain and/or disability due to a wide range of reasons. I also am affiliated with UC Davis, Dignity Methods Family Medicine and Sierra Nevada Memorial Hospital and a clinical and research mentor for medical students and residents.
To give a little background, I took an unconventional path to where I am today and, having lived and practiced medicine in multiple countries has caused me to continuously question and reflect upon even my most deeply-held personal, cultural and scientific beliefs. Questioning the popular narrative has become a foundational part of who I am. I started college as a French and English major at UW Madison wanting to be a musician or writer but, while studying philosophy and film at the University of Paris, a German internal medicine resident convinced me to go back to the US to go to medical school so I could become more globally employable. It was great advice! The pre-med coursework was delightfully objective and I could not believe how much I loved calculus and organic chemistry. Medical school was a wonderful experience and medicine is to me the best profession in the world. There is no better way to truly connect with our fellow humans. During medical school, I matched into (my first choice!) ophthalmology residency, but when I learned I was pregnant and was offered an inflexible 15 days of maternity leave (at that time I was living alone) and medical and nanny bills I would never be able to afford, I decided instead to move to Denmark with my Danish soon-to-be husband. Getting approval to work as a physician in Denmark was something… I ended up learning Danish and passing all the required medical school tests in about six weeks (with the required score of 100% on all the tests for non-European medical grads), just so I could start earning money. After a few months, the hospital I was working in encouraged me to apply for the MD specific PhD program given the background I already had doing aging research at Harvard. They were starting a large population-based study and wanted me to run a portion of it, which I ended up doing. This earned me a PhD in Epidemiology and Public Health from the University of Copenhagen (yes, the courses are in Danish) and I went on to do related post-doctoral work. To the physicians reading this, I need to explain that MD, PhD students are paid a real physician’s salary while they do their PhD and there are 9 months paid maternity leave, supplemented childcare and lots of paid vacation time. On top of this my PhD advisor was the best and has a dual appointment at University of Copenhagen and Harvard so I felt like I had really beaten the system.
In 2015, our family moved to California I did my residency at UC Davis and my husband was offered a job in the Heme Onc Department at UC Davis so it was a sort of couples match. I had become connected with UC Davis through my research on vision loss in long-distance runners. This was a condition that Marty Hoffman, Kim Corrigan and I originally defined in 2015. I have done a lot of research in the physiological effects of ultramarathon running and wrote as the columnist “Ultra Doc” for UltraRunning Magazine for the past two years. I actually used to work as a semi-pro athlete for Salomon and ran on the US and Danish national teams in ultra and mountain running. But relevant here, from early on in the pandemic, I worked on epidemiological research to help fill in the gaps in our knowledge especially about COVID-19 in children. I felt compelled to get involved in this because of what I was witnessing happening to my own children and their friends especially considering the discrepancy between US and Danish policies around children and schools. I have testified twice before congress about school closures and COVID-19 in children and served as the medical advisor for a large K-12 diocese in Northern California which was able to stay open the entire 2020-2021 school year for in-person learning.
My favorite substack yet! I want to forward this to every physician in my multi-specialty group!! My lowest point in the pandemic came discussing the risk benefit analysis for a young healthy patient who was in tears because her college mandated a booster dose for her to return to campus. I spoke to the physician at the college on her behalf. He insisted I didn’t understand how high her risk was despite already being vaccinated at 20 years old without any medical problems.
Everyone should read this!!! Thank you, Dr. Prasad and Dr. Hoeg! We appreciate all your hard work!