
Why you should NOT get a whole body MRI
Even if it & all downstream testing were free, I would say no. It is a bad idea.

There is a debate online about whether or not it is paternalistic for doctors to counsel patients against getting a whole body MRI from services like Prenuvo. The arguments drift towards cost and who should pay for further workup, but what if the test and all downstream procedures were free? What if we focused just on the health impact? Should you get a whole body MRI? Would I? Why not?

How you feel about the question depends heavily on your model of cancer. Most people think that cancer starts in a target organ (the breast or lung), grows for a while, and then sheds it cells into the blood (or lymphatics) and spreads. Most people think that we can cure cancer when it it is localized, but can’t when it spreads. They think our treatments for cancer that has spread are toxic and barbaric and anything you can do to avoid that is beneficial.
Based on this worldview, any tumor you find that hasn’t spread is a life saved. Millions have had tumors found by mammograms or PSA screening, and feel like they were saved. As such, screening is good. What’s the worst that could happen, you get a false scare, but are reassured later? That’s preferable to the alternative or missing a tumor and dying as a result.
The problem is that this model of cancer is naive and incorrect. I am going to offer a richer model, but I am also going to simplify so it is understandable. Imagine there are 3 types of tumors. They all look like the same cancer under the microscope.
All tumors start in a target organ (breast, lung or colon). The first grow slowly and are unlikely to shed cells elsewhere. These are not going to kill you in your natural life. You might feel them with your hand someday and cut them out, but even if you didn’t, you have nothing to worry about.
The second are those that spread microscopic cells very early on. Even if you find them when small, they have seeded other organs. There is almost nothing you can do to avoid dying by this cancer short of removing all your organs prophylactically— but then you have other issues. If you find this tumor and cut it out and take chemo— you still die of that cancer— but with a few more surgeries and more time on chemo than had you found it later.
The third type of tumor is the tumor that starts in the target organ, and was going to spread, and going to kill you, but because you find it and cut it out, you live much longer than you otherwise would. This is what we want to find!
Now consider that all three are indistinguishable under the microscope. All get the same treatment— surgery, radiation, and chemotherapy.
The problem is that finding tumors #1 and #2 is not good for you. You are subject to surgery, radiation and chemotherapy that you don’t need. These interventions can improve survival when done appropriately, but when done on people who don’t need them, result in a net loss of survival. Your life is shorter and worse off if you got these treatments when you can’t benefit.
Finding #3 is great, and I wish we could find selectively.
What does whole body MRI find?
The answer is we have no fucking clue what tumors will be found by whole body MRI. Are we more likely to find #3s or are we finding mostly #1s and #2? IF you find too many of the first two, you might actually shorten survival.
We are probably not finding #3s
The thing experts in cancer screening know is that finding #3s is challenging, and our efforts to screen for cancer are a total failure. No cancer screening test has ever shown overall survival or even all cancer death benefits in a randomized trial. CT screening for lung CA briefly did in NSLT, but that was noise and lost when Pinsky re-examined it.
All proven cancer screening tests have limited impact on cause specific mortality. Meaning that we mostly don’t find #3s. This is from my paper. Deaths NOT SAVED is the dominant category.
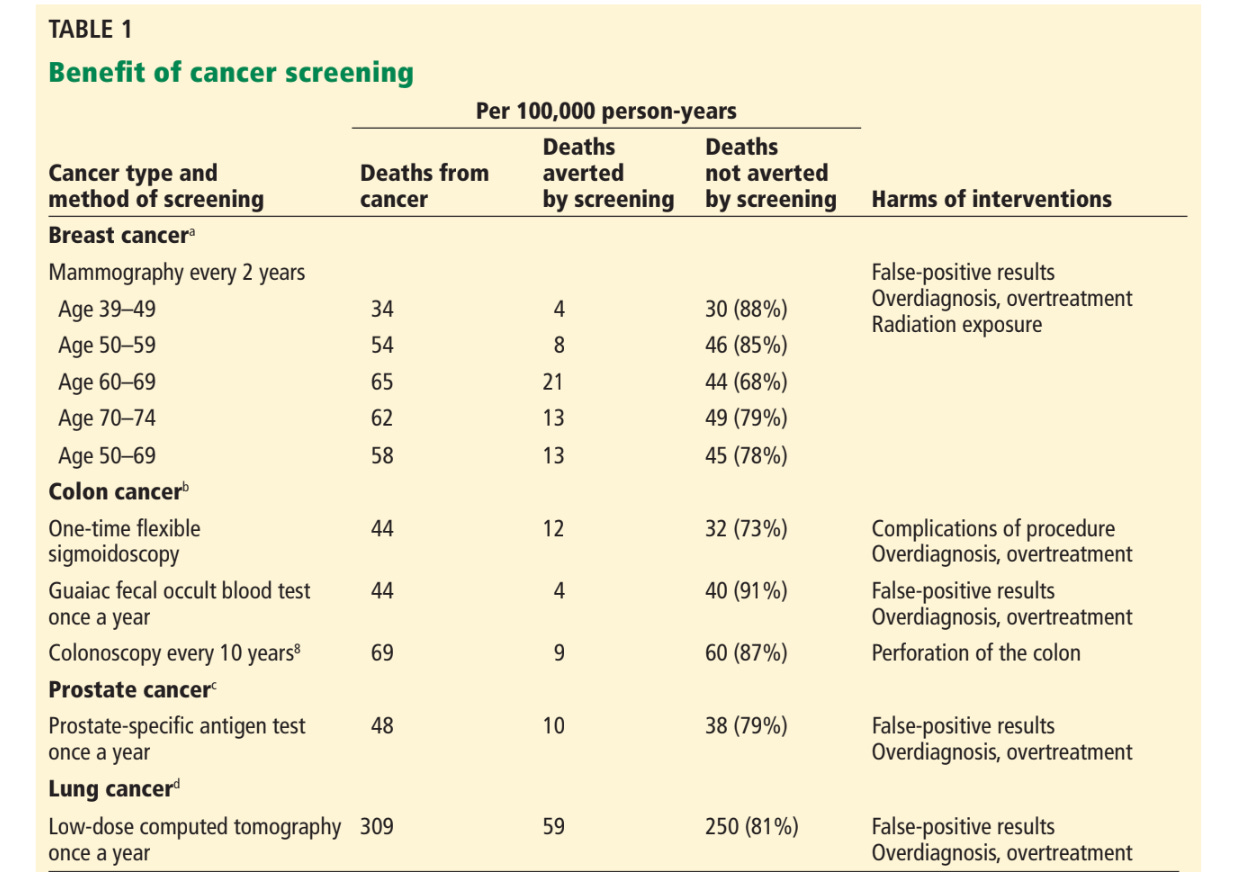
Finally, all screening tests have a high rate of number needed to diagnose— number of people who undergo treatment to avert one death. Even in the positive PSA trials, this number is in the high 20s. Thats a lot of over-treatment.
Finally, MRI looks at tissues known for indolent biology (e.g the thyroid, the adrenals, the kidneys), if anything it might perform worse than mammography. For these reasons, I worry that MRI screening is much more likely to find #1s than #3s, and I would need data to convince me otherwise.
The toxicity from treating people who don’t benefit adds up
Chemotherapy that you don’t need isn’t a good thing. The only thing worse is living in a delusion where you thought you needed it. Chemo increases the risk of secondary cancers. Getting radiation and surgery that you don’t need is also harmful. These things will increase death rates. It doesn’t take much of an increase in these off target deaths to negate any benefit from screening.
Why it is more complicated than this?
The truth is more complicated because some tumors don’t cause harm even if they spread, and that the counterfactual where you don’t find it on scan x is not always not finding it, but finding it as you might otherwise (with your finger or a some symptom). Screening is always against the backdrop of life in America, and must show benefits above and beyond normal life. But even with a more complex model— which is how I think about cancer— screening falls short without hard data.
Why I won’t do it?
Arrogant people have tried doing things to healthy people to make them better off for thousands of years. Nearly none of these people did any good, and the majority did more harm than good. Modern AI and tech researchers are not much smarter than our ancestors. They are just as arrogant (perhaps more so), and probably getting this wrong.
How to validate Prenuvo
The only difference is now we know the definitive experiment to see who is right. A randomized trial powered for all cause mortality. Take 250,000 people and put half in the whole body MRI and let the others live normally, and see if they live longer. If you think this takes too long, crank up the sample size to 10 million. (PS the median need not be reached for OS to be shown), and it will result sooner.
Why doesn’t the FDA demand proper data from GRAIL and prenuvo?
Expecting the FDA to do the right thing is even more foolish than thinking Prenuvo helps. The FDA approved covid 19 shots and boosters for babies based on no credible data; They are approving Alzheimers drugs that don’t work. Postpartum depression drugs that are dangerous, and cancer drugs that don’t work. The agency is run by people who are not good at evidence based medicine (Peter Marks, Rick Pazdur, Bob Califf), and under tremendous political pressure to approve products so that politicians get more donations. Most FDA employees work for the industry when they leave. I don’t expect much from them.
Closing thoughts
I want to address this final comment.

Most people in healthcare and technology don’t understand screening. They haven’t studied it, and have a poor understanding of cancer.
If you want to learn more about cancer screening; here are the 17 articles I have written on the topic over the last decade. Free access. If you like analysis like this, subscribe
The older I get (early 70s) the more wary I am of all these tests--especially mammo-- for exactly this reason. Yet one is led to believe that avoiding them is un-American, incredibly risky, and will piss your doctors off such that the doctor-patient relationship is seriously undermined. I'm always looking for doctors that do not "go by the book" as one once told me. Who are open to being flexible about association-mandated testing and pharmaceutical therapies. But I understand that doctors are evaluated on how many of their patients conform to these norms, they are overwhelmed and worried about being sued for missing something, and just want to get through the day without having to have a big discussion about the DEXA or the mammo. It's really hard to decide what to do--or not do. I've been putting off the mammo and screening pelvic ultrasound for the last year or so, having been lucky enough to never need further testing so far over my many years of these tests. Most people think I'm nuts: What? Just get your mammo!
I had a kidney "incidentaloma" in 2009. Complications from the surgery to remove it were life-threatening. Only afterward did I read Dr. H. Gilbert Welch's "Overdiagnosed" which makes the same points you are. Between 1975 and 2005 yearly kidney cancer diagnoses went from 7000 to 13,000 per 100k. Presumably all those diagnoses led to an intervention. Deaths went from roughly 4000 to....4000. So we can conclude NONE of those interventions, on average, led to saving any lives.