
Peter Marks' FDA is Playing Games with Young Men's Health & Maximizing Pfizer's Profits
3 pieces of data from this week.

I want to present 3 pieces of data which continue to build the case that this FDA, under Peter Marks, is acting recklessly with its push to boost, in perpetuity, 18 year old men who had COVID19.
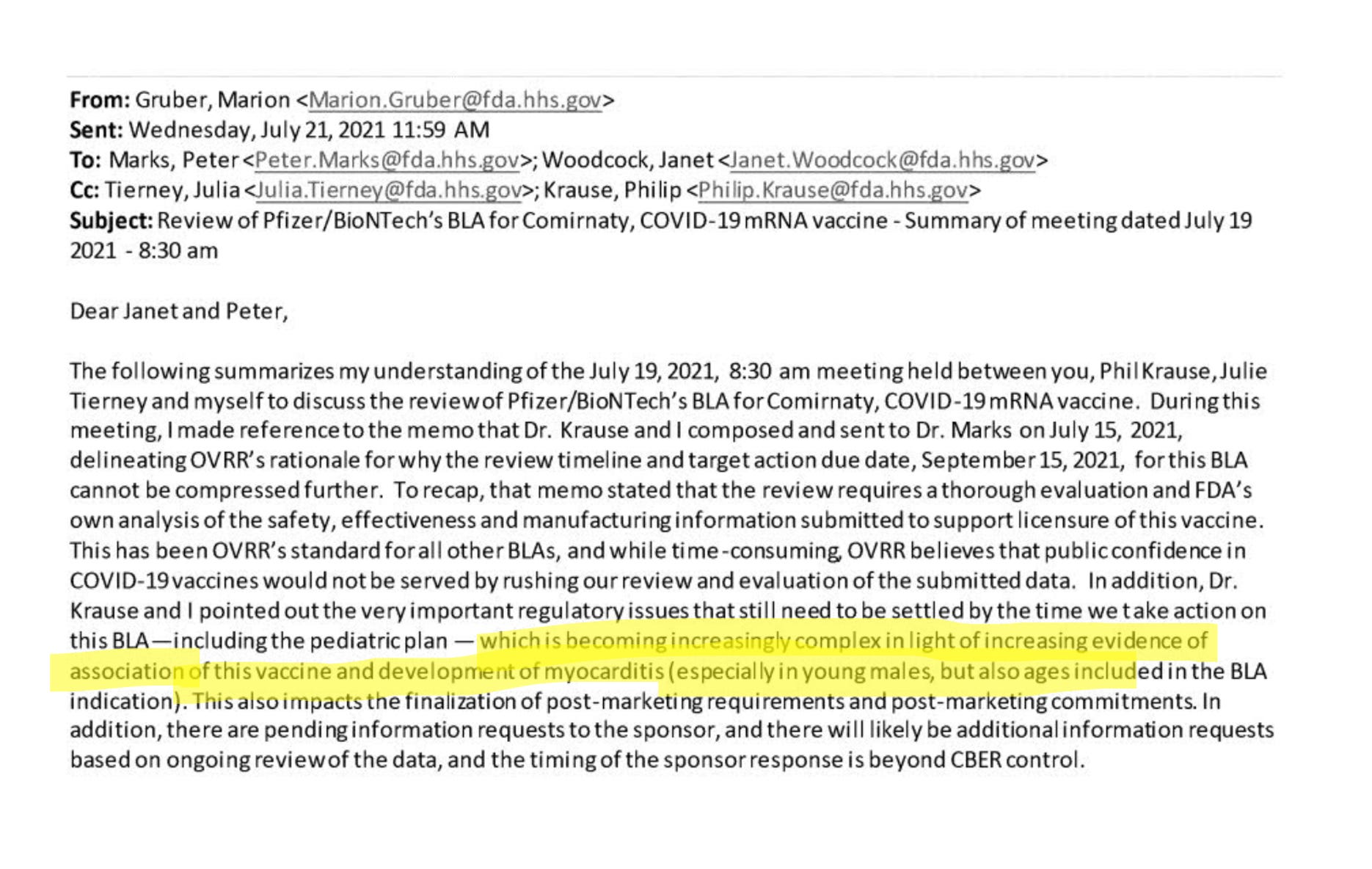
This week, internal emails show Marion Gruber, former head of FDA vaccine science frustrated with Marks. She specifically highlighted the myocarditis issue. Myocarditis appears to occur at least 1/10k with boosters, and subclinical troponin elevation is likely 100 times as high (based on 2 studies). This concern was ignored.
FDA under Marks has changed the date Pfizer is required to turn in postmarket safety data. From Dec to June. This is the study to look for troponin in young men. These data were needed in 2021— their continued delay is catastrophic.
 Jessica Adams@RxRegA#VRBPAC It appears FDA has extended the due date for Pfizer's subclinical #myocarditis substudy that was a condition of approval to Jun 2023 from Dec 2022, a change made since I last checked the website on Jan 23. H/T @walidgellad! accessdata.fda.gov/scripts/cder/p… fda.gov/media/151710/d…
Jessica Adams@RxRegA#VRBPAC It appears FDA has extended the due date for Pfizer's subclinical #myocarditis substudy that was a condition of approval to Jun 2023 from Dec 2022, a change made since I last checked the website on Jan 23. H/T @walidgellad! accessdata.fda.gov/scripts/cder/p… fda.gov/media/151710/d…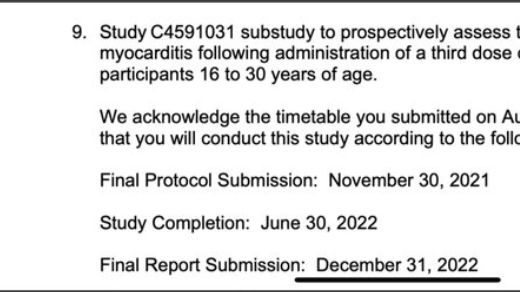
 Jessica Adams @RxRegA@rfsquared @US_FDA @pfizer @DrPaulOffit On #9 the question is simple: What was the incidence of subclinical myocarditis following administration of a third dose in a subset of participants 16 to 30 years of age? TY @IamBrookJackson for sharing this nifty website: https://t.co/V5mncKgLEs https://t.co/8cS0TFOtbs12:02 PM · Jan 26, 202323 Reposts · 43 Likes
Jessica Adams @RxRegA@rfsquared @US_FDA @pfizer @DrPaulOffit On #9 the question is simple: What was the incidence of subclinical myocarditis following administration of a third dose in a subset of participants 16 to 30 years of age? TY @IamBrookJackson for sharing this nifty website: https://t.co/V5mncKgLEs https://t.co/8cS0TFOtbs12:02 PM · Jan 26, 202323 Reposts · 43 LikesIt is now clear that bivalent boosters also have myocarditis; from today’s VRBAC
If the rate of myocarditis is 1/10k hospitalized (consistent with Sharff’s estimate for the last booster), how can the benefit outweigh this in a 16 year old man who had COVID? He does not have even an absolute risk of 1 in 10k hospitalization from reinfection. This is now a harmful intervention until proven otherwise.
Nicole Saphier, MD@NBSaphierMDVRBAC: Signal detected for increased myocarditis/pericarditis following bivalent booster among 18-35 year olds, similar to old vaccine. There is no reason to recommend a booster in healthy younger individuals, to do so is negligent. 3:42 PM · Jan 26, 2023182 Reposts · 570 Likes
3:42 PM · Jan 26, 2023182 Reposts · 570 Likes


Peter Marks has eliminated all dissenting voices at FDA and is hellbent on sacrificing evidence based medicine in an effort to give Pfizer a perpetual market share in young people. If he were at FDA instead of Frances Kelsey, thalidomide would still be a treatment for morning sickness.
Oh my god guys, this is so upsetting. I have met Marion Gruber while working on regulatory issues around FMT (fecal transplants). She always struck me as very smart, dedicated and by the book. She had the hardest questions but was genuinely someone I could respect. Peter Marks seemed like more of a bully and jerk in person (sorry, my impression). Anyway, the decision to regulate FMT as a "drug" rather than stool banks (perfectly safe and cheaper) told me everything I needed to know about loyalties to industry rather than doctors/patients.
No matter what data comes out or how sketchy this all seems, most of my colleagues seem completely unreachable, like invasion of the body snatchers. I try to tell people and share on my facebook, etc and it's the same few who comment/care. Now my hospital system requiring booster of every employeed. I wrote a very well considered and referenced email to the head of infection control and didn't even get a response. One trainee I discussed this with gave me a blank look and said "I just follow guidelines and don't think about things like that." I am worried on so many levels: for my own kids-who may have forced mandates when they start college next year, for my patients, for myself (donated kidney in november and now seeing AKI data from New Zealand), and most of all for what has happened to the profession that I have dedicated my life to.
Another frustrating thing the government does when comparing myocarditis risk due to Covid versus myocarditis risk from mRNA vaccination is that it’s a false comparison given that vaccination doesn’t prevent infection. It would be a valid question if vaccination prevented infection but many young people have been infected and vaccinated and will almost certainly get infected multiple times in the future. There is no point in risking myocarditis via vaccination without a benefit that exceeds the risk.