
What is the truth about alcohol consumption
I take a deep dive into the question: How much alcohol should a person drink?

Right now, you are someone who drinks 0, 1, 2, 3 or more drinks a day. These drinks might be tequila neat, Mad dog 20-20, an Oakville, Napa cabernet, or Bud Lite. Probably, you are not consistent. You might drink 1, 2 or 4 nights a week. You might drink before meals, or after dinner. You might drink a hazy IPA after a long run, a Corona after mowing your lawn, or sip a gin and tonic on a hot summer day.
Some of you are wondering if your habits are healthy— or should you drink fewer or perhaps more drinks? And what if you are starting from scratch: say you are a 16 year old who hasn’t yet had a drink, but thinking about it. Should you start?
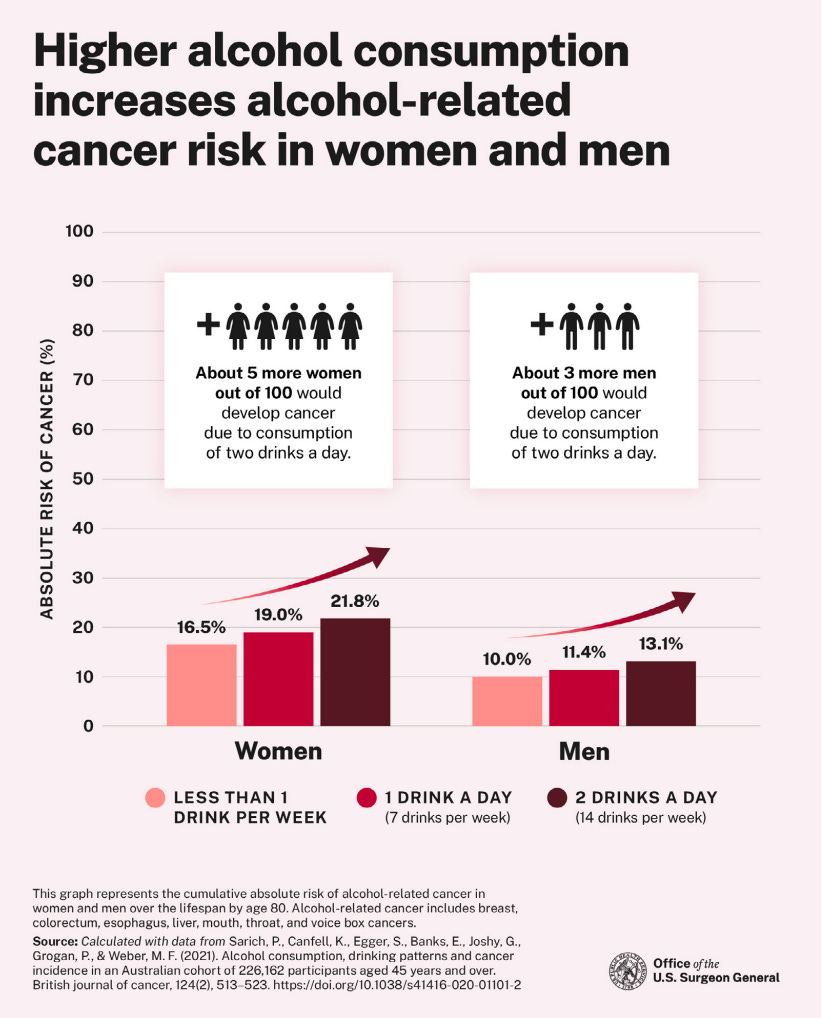
The Surgeon General put out advice saying that even moderate drinking is linked to a series of cancers. He says at least 7 cancers are implicated.

He wants a warning on alcohol. Is that a good public policy decision? Is it supported by evidence?
In this essay, I will outline the evidence on alcohol. I will start with a large meta-analysis and then explore the underlying observational data. I will discuss the mechanistic science. I will provide a study that I think the US NIH should fund that will provide guidance, and finally I will end with my alcohol recommendations. Am I evidence based? I will end with a meditation on that question.
If you believe in what I am doing, please become a subscriber.
Let’s begin with the large studies
Many authors, including the economist Emily Oster, whom I respect as a sound and logical thinker, cite this Lancet paper, as evidence alcohol is harmful. (Oster writes, “my read of the evidence is that alcohol isn’t especially good for your health”). Let’s take a look.

These are some figures that Oster highlighted


(Note the protective effect on heart disease)
Is this paper credible?
A meta-analysis is like a juicer, it only tastes as good as what you put in. This study takes data from many nations, standardizes alcohol consumption and standardizes endpoints. But what is the quality of the underlying data? I decided to select one, large, recent US based study to provide a litmus test. I asked a scientist who runs my epidemiology laboratory at UCSF to send me a randomly chosen, recent, US based study, just as a litmus test. She sent this.

I then read this paper, here are just a few issues with it that jumped out at me on first read.
Alcohol intake is self-reported (there may be huge errors of over and underestimation and these may vary by race, socioeconomic status, and education. None of this is considered).
People who don’t drink is a motley crew of those who don’t for health reasons, those who don’t because they have a drinking problem/ or were told not to drink because they have cirrhosis or other malady. The authors try to solve this problem by breaking people into never, former, and infrequent drinkers.

The authors define “never drinkers” as those who didn’t drink in the last year, and have never had more than 12 drinks in their life. The number 12 has no justification. Former drinkers had 12 or more drinks in ANY previous year, but none in the last year. Former drinkers also had to drink more than 12 drinks lifetime, but this is a silly thing to say because if you drank 12 or more in any prior year, you, by definition, have drunk 12 or more lifetime. Do they authors realize this redundancy? Lifetime infrequent drinkers were 12 or more lifetime, but fewer than 12 in any previous year. I find this definition a little nutty. You could drink 30 drinks a day for years, but if you spend a year in Tibet, you get called lifetime infrequent.
Presumably a cirrhotic patient or someone with a drinking problem would fall into Former drinkers category, but also someone who had a single fun year in college. And let us be clear, never drinkers are ONLY a SUBSET of people we would call non-drinkers. They had to be a particularly odd group in college. They drank fewer than 12 in all those years. And here is what light, moderate and heavier drinkers mean. Heavy drinking is a glass of wine a night in women, but also a fifth of vodka a night. A crazy meaningless bucket term.

Shitty definitions show these are confounded groups. Already above you can see these definitions define wildly different groups of people. Take a look.

Former drinkers are 12 years older than never drinkers. People who went to college drink more and drank more. Look at the racial differences. It is a fucking mess of confounding. An economist running a natural experiment would shit their pants with data like this.
They have no data on socioeconomic status (income or wealth)
They have no ability to differentiate drinking Bordeaux or Mad Dog 2020
They find links to cancer mortality. For example, smoking is linked to lung cancer. in the total cohort, but when they restrict to never smokers, the effect vanishes.


This result stinks of residual confounding. Drinkers also smoke. The authors are adjusting for smoking only by tertile of use, which is a crude adjustment, there is like more unadjusted smoking there analysis and this stratification proves it.
At times, the authors find things that undermine their message.

But for this they say:


Why are these data not shown?
The authors don’t adjust for getting mammograms.

Getting a mammo is linked to SES and education, and nothing finds more cancer than mammos. They authors fail to adjust for this. See work by Welch

The study is asking if alcohol use is linked to cancer mortality, but not whether changing one’s alcohol use reduces cancer. One can imagine a target trial observational analysis (ala Hernan) that tackles the salient causal question. Should I adjust my intake?
In addition to type of alcohol, quality of alcohol, the authors don’t have a way to measure how fast or slow people drink, with or without food, with or without company, what time of day they drink, whether they sleep or eat well otherwise, whether exercise modifies the effect, and many other salient questions.
The authors find bizarre things like this

Now, the definition changes. This is by days per week not light, moderate and heavy. Why is that? Also are you saying that I lower my risk of prostate cancer by drinking more on Friday if I drank Weds and Thursday? A implausible conclusion.
Overall, this paper is emblematic of the literature. Old data. Shitty data. Confounded data. Weak definitions. Measurement error. Multplicity. Time zero problems. And illogical results. Calling this paper science is a stretch. Belief in it’s results has more in common with religion.
The meta-analysis is a collection of studies like this. It looks fancy and cool, but it is putting a bunch of rotting fruit in a juicer and calling it a smoothie.
Mechanistic science
The surgeon general has this to say to about how alcohol causes cancer. I find it unpersuasive. Let’s consider why.

First, of all, it is unclear to me how many of these studies reflect what happens in vivo with modest (e.g. 2-4 glasses of wine a night). Second, this type of mechanistic science applies to every single drug in pre-clinical testing, 9999/10000 don’t come to market (aka the mechanism fails) despite having robust “mechanistic logic.” Next, you can read dozens of papers telling you the mechanism of action of Ivermectin in COVID, or remdesivir.

And here is the mechanism of action of cloth masks, though we have direct, cluster randomized data these don’t do shit.
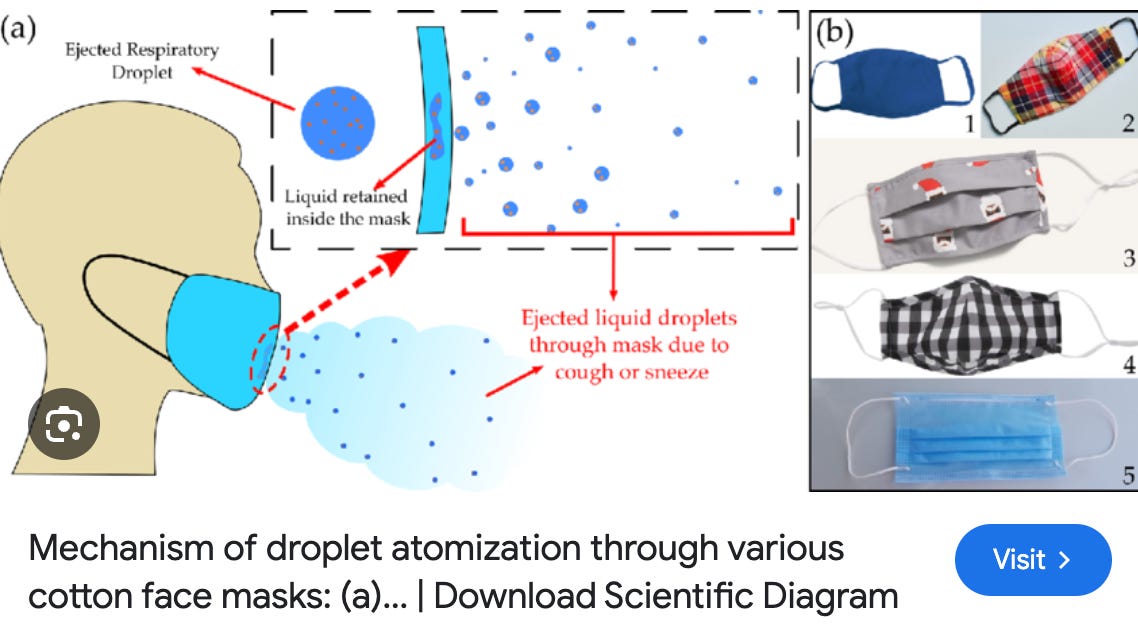
Bioplausibility or mechanism of action is notoriously unreliable to know the effects of a substance in people. Particularly something with complex social and behavioral impacts like drinking alcohol. I put bioplausibility studies in the circular file.
What would settle the alcohol debate?
Previously, in these pages, I describe the way to settle the alcohol debate, and I will summarize that here

Your support keeps this stack going against all the powers that be.
First, it is important to consider ALL THE ENDPOINTS. A healthy person cares about the totality of health. I think at least 4 endpoints are relevant
How long will I live?
How well will I live (morbidity/ disability)?
How happy will I be/ How will I feel?
How happy are people around me/ How will they feel?
If alcohol lowers ischemic heart disease, but increases cancer (PS I doubt both these claims), we have to take both into account. The Surgeon General famously evades such a calculus. Next, where is the consideration of the pleasure of alcohol? And of course, alcohol can make some people a terrible companion, but it also improves others into being more vivacious and outgoing. There is a good reason so many dates, dinners and parties involve alcohol.
So I propose a multi-arm randomized trial (Please note, there are formal designs of such studies). From my original essay
We enroll people with their current preferred baseline drinking (0,1,2,3,4, etc.). We randomize them into one of 7 arms.
Arm 1: Stay the course
Arm 2: Decrease your drinking by 1 drink a day (advice given)
Arm 3: Increase your drinking by 1 drink a day
Arm 4: Decrease your drinking by 2
Arm 5: Increase your drinking by 2
Arm 6: Stop all drinking
Arm 7: Carpe diem (only advice provided)
Then, we follow people into the future. First, we measure the impact of our intervention on drinks consumed. Of course, like all complex social behavioral interventions, we won’t have perfect compliance, and that is ok. Our policy tests whether one recommendation is preferable to another. First step is to see what delta (drink consumption) we get from recommendations.
Next, we follow people into the future and look at all the relevant endpoints. If we enroll many people 65+, we may, in a few years, have some mortality data. I suspect it will generally be null. We may also have disability data (related to strokes, suicides, etc.). Again it is likely to be null.
[We can also measure things like rate of divorce]
But the two most important endpoints: How you feel about your life, and how others feel about you will be continually captured. We will provide surveys to individuals, or have a diary tracking mood.
Because it is difficult for modest changes in nutrition to change duration of life and disability, the last 2 endpoints will likely drive the entire study (I.e will provide the most information to help you).
A large, multi-arm RCT is the only path forward. In fact the NIH almost ran one. Before he was smearing scientists who were correct on lockdown and school closure, Francis Collins almost did this.

Now that Jay is headed for the NIH, the time is perfect for a large, 15 year, 250 million dollar, NIH funded (not Jose Cuervo funded) trial of alcohol. A randomized trial will be a lamp in this cave of darkness.
Short of that, the best studies are likely those where an economic crash changes alcohol consumption, or the effect of new alcohol tax, or other natural experiment. Ultimately, these are imprecise however and there is no substitute for randomization.
While we push for such a study….
What are my recommendations for drinking alcohol? And am I evidence based?
First, let me give you my principles for alcohol. The advice I tell friends and family.
1 Parents should introduce their kids to alcohol before they go to college. Ideally good wine with dinner, properly paired. First introduction should not be a frat party.
2 Never drink a drink you don't like. If it's poorly made, or you hate it, don't drink it. Throw it away.
3 Don't count your drinks. That's antithetical to the pleasure of drinking, and a buzz kill.
4 The best drink is the one immediately before dinner.
5 Good food should be served with good wine or beer, as appropriate. Brandy and sherry at the end of a meal.
6 Jalapenos and habaneros have no business in alcohol.
7 Don't drink and watch TV.
8 Don't drink alone, unless you're meeting someone later and need liquid encouragement.
9 Learn how Beer, Wine, and Scotch are made. For drinks you like, learn how they are made. Learn to mix good cocktails. You should know at least 25 off the top of your head.
10 Pour a bunch of drinks, for instance, several types of whiskey or wine, and learn to appreciate the differences. Do it with a blindfold on. Don’t say peaty, unless you know what that means.
If you love red wine take Sommelier training.
Have your last drink at least an hour before bed.
You can come to my dinner party and not drink, but you won’t be coming back.
If you wake up with headaches and can’t work/ call in sick, you have a drinking problem and should cut back or cease.
If you are having outburst at your children or spouse, same as above.
Drink with friends. Drinks pair best with laughter.
Marijuana when used in moderation can reduce alcohol consumption.
If you have acetaldehyde dehydrogenase deficiency, don’t drink. This cancer risk is insane. Use marijuana instead. THC soda’s if you want.
If you like red wine, put 6 bottles (at varying price points 10-200 dollars) of the same grape (e.g. Cabernet or Syrah or Petit Verdot) in paper bags, hide the label, open all 6. Let everyone try all the wines, and write down notes on taste. Try to guess the prices.
A long run deserves a cold beer.
Alcohol should be thought of like other foods. There are reason why some alcohol is served before meals, with steak, with dessert, by the fireplace. These traditions can include the chemical properties of fatty red meat and the tannins in red wine. These should be learnt and understood.
You can learn more about alcohol from a chef than an epidemiologist. And more from a Sommelier than the Surgeon General.
People who don’t drink because they seek longevity will likely live a short, miserable life.
Some people tell me they feel bad when they drink, what should they do? Well, if you don’t even like drinking than don’t do it, but perhaps there are things you haven’t learned about wine and spirits.
As yourself if you know what “Terroir” means with respect to wine. If no, then there is a lot to learn in this life.
Read this…
Are my recommendations evidence based?
Some of my recommendations are serious and some are tongue in cheek and that is intentional. Evidence is inadequate for many major life choices. Who should you marry? Should you eat Italian food or Indian food for dinner? Is it better to to drink red or white wine with steak? Ok, that’s easy, obviously a full bodied red wine served at 65 degrees.
Alcohol and humanity are intertwined in ways far beyond medicine. There are spiritual, emotional, humanistic, cultural forces at play. It is profoundly American to ask should I drink a glass of red wine a night to maximize my lifespan. You would be much better off going to Italy for 6 months, shutting the fuck up, and doing what they do.
We deserve a series of simple, elegant, multi-arm randomized trials of alcohol. We can easily get the money for this by firing the legions of retrospective observational epidemiologists who give science a bad name.
While we wait for this, we should have humility. The surgeon general is not chosen based on merit and should not be deferred to. Medicine has no business advising people when it doesn’t have robust data. This spills credibility. The report was his swan song to recommendations without good evidence.
If you don’t want to drink, no one is forcing you (well, unless you want to be invited back to my dinner party). If it affects your work or family, you have a problem, but if you enjoy it, study it, and pair it with food, fire, and company, then I will cheers to you.
If you liked reading this, and appreciate my perspective, subscribe
“You can come to my dinner party and not drink, but you won’t be coming back.”
Wow. No what I would’ve expected from a mature person. It appears you think drinking is required to be socially accretive. Weak sauce.
So glad you addressed this! I’m not a big drinker (2 glasses of anything, and I’m sawing logs), but I wondered why this Prohibition style document suddenly appeared and what evidence arose to spark the alarm. I’m glad to have your take. And I am particularly delighted with your sense of humor. I had no idea when I first saw you on ZDogg back in the beginnings of the wet-market nightmare that you were this irreverent and hilarious. Who would have thought that evidence-based medicine could be so much fun!